Effects of a Forest Therapy Program on Reducing PTSD and Depression and Improving Mood States in Fire Officers
Article information

Abstract
Background and objective
This study was conducted to investigate the effects of forest therapy programs on reducing post-traumatic stress disorder (PTSD), depression and improving mood states in fire officers.
Methods
To determine PTSD, depression, and mood states before and after the forest therapy program, the survey results of 185 fire officers were analyzed. Frequency analysis was conducted to identify the demographic characteristics of the participants, and Wilcoxon signed-rank test to analyze the differences among group.
Results
As a result of a comparative analysis of PTSD before and after the program, there was a significant decrease in PTSD from 10.65 ± 12.00 to 5.64 ± 8.29 after the program. Depression also showed a statistically significant difference from 3.21 ± 4.00 to 2.21 ± 3.47 after the program. As a result of comparatively analyzing mood states before and after the program, there was an increase in positive factors and a decrease in negative factors. Total mood disturbance (TMD) also showed a statistically significant decrease from 5.78 ± 17.37 to –7.38 ± 10.35 after the program.
Conclusion
This study has significance in verifying that forest therapy programs can bring psychological changes to fire officers, and these results can be used as a basis for stress management and relief of fire officers.
Introduction
Despite the rapid industrialization and urbanization of the modern society, the scale and pattern of disasters or accidents rather turn out to be unpredictable regardless of development size and changing speed (Jang, 2018). We are constantly surrounded by accidents and incidents, such as the Sewol ferry disaster in Jindo, Jeonnam in April 2014, the sports center fire in Jecheon, Chungbuk in December 2017, the fire at Sejong Hospital located in Miryang, Gyeongnam in January 2018, and the massive forest fire in Goseong, Gangwon-do in April 2019. Fire officers are always on the front line of these accidents and incidents.
In fact, according to the statistical data announced by the National Fire Agency (2020), the number of reports sending fire officers to the scenes increased by approximately 18% from 756,987 cases in 2016 to 893,606 cases in 2019, and the number of rescues is also continuously increasing every year, from 609,211 cases (2016) to 655,485 cases (2017), 663,526 cases (2018), and 719,228 cases (2019). This implies that accidents and incidents happen frequently in the communities. Fire officers working on the front line of these accidents and incidents with physical risks are exposed to stress caused by shocking and terrible scenes almost every day. The National Fire Agency (2019) conducted a survey among fire officers on four major types of stress such as post-traumatic stress disorder (PTSD), depression, sleep disorder, and alcohol use disorder. As a result, 2,453 (4.9%) out of 48,098 respondents were classified as those at risk of suicide, and 53 (0.1%) fire officers responded that they conducted self-injurious behaviors with the intention to die. The survey results showed that 54.7% had PTSD, 81.1% had sleep disorder, 62.3% had alcohol use disorder, and 67.9% had depression, showing 2–3 times higher rates than the entire average. In particular, the rate of PTSD was 10 times higher, indicating the need for more intensive management. To prepare for external harmful factors that occur at the scene, fire officers must reduce physical and mental stress and enhance resilience for management in everyday life.
Many studies are conducted on forest therapy to promote stress management and health of people today suffering from physical and mental health problems caused by being exposed to all kinds of stress in the social environment. Forest therapy programs for workers engaged in emotional labor had a positive effect on stress management and emotional change (Lee et al., 2018), and also a positive effect on physical health recovery and life satisfaction of middle-aged women (Kim, 2020). Forest therapy programs also positively improved the attitudes of adolescents under probation toward forests and reduced their anger (Kim et al., 2020), while relieving stress and increasing self-esteem of cancer patients (Kim, 2020). As such, forest therapy programs using forests have various psychologically and physiologically positive effects on the human body. Korea Forest Service is providing forest welfare services for the people to promote national health and improve the quality of life. These forest welfare services are provided for all ages throughout the entire life cycle from early childhood, adolescence, middle age, and elderly, as well as pregnancy. There are also programs considering the characteristics of the beneficiaries with special needs, such as underprivileged people, traumatized families, children of North Korean defectors, and maritime police, thereby contributing to promoting national health and improving the quality of life.
This study determines the effect of the forest therapy program carried out for 5 days and 4 nights on reducing PTSD and depression and improving mood state of fire officers, who have the occupational characteristic of having to be at the scene handling dangerous and urgent accidents and incidents and work in shifts that may cause imbalance to the biorhythms.
Research Methods
Study sites and participants
The study site is the National Center for Forest Therapy with the area of total 2,889 ha in Yeongju-si and Yecheon-gun, Gyeongsangbuk-do (Fig. 1). The area of the central district is 142 ha, featuring a health promotion center for health measurements and indoor therapy equipment, accommodations for about 600 visitors to stay for short-term or long-term visits, and a hydrotherapy center to experience a hydrotherapy program using all kinds of water pressure massages and spa facilities. There are 9 major forest paths about 45 km long including barrier-free decks in universal design for the elderly or the disabled to use conveniently, an anion therapy garden next to a valley, and an aromatherapy garden with over 100 thousand Korean native plants in 64 species. There are also various gardens and facilities such as a barefoot healing garden made with natural materials like wood chips and gravel to step on, as well as a Korean medicine exhibition garden where medicinal plants are planted. In Yecheon-gun, there is also a forest therapy culture center, a specialized facility for tea ceremony and meditation programs.

The location of research site.
The participants of this study are fire officers that visited the National Center for Forest Therapy for about 8 months from March to November 2019. Total 268 fire officers participated in the 5-day, 4-night Stress Resilience Enhancement Program in 9 sessions. The fire officers responded to the survey and measured their physical health before and after the program. Prior to the survey, we explained the purpose and contents of this study and received their consent to participate and use their personal information. A self-report survey method was used to determine their post-traumatic stress disorder (PTSD), depression, and mood states, and effects analysis was conducted on only the experimental group.
Tools
PTSD (post-traumatic stress disorder)
To measure the PTSD of fire officers, the Korean version of the PTSD Checklist (PCL-5-K) was conducted before and after the Stress Resilience Enhancement Program. The PCL-5-K is a self-report survey measuring the existence and severity of PTSD symptoms, comprised of total 20 items developed by Weathers et al. (2013) and adapted in Korean by Kim et al. (2017). The items are rated on a 5-point Likert scale: ‘Not at all (0 points)’, ‘A little bit (1 point)’, ‘Moderately (2 points)’, ‘Quite a bit (3 points)’, and ‘Extremely (4 points)’. The scores range from 0 to 80, with higher scores indicating more severe PTSD. The cut-point of PTSD is 33 (National Center for PTSD, USA). Cronbach’s α was 0.94 at the point of the tool development, and Cronbach’s α in this study was 0.95.
Depression
To measure the depression levels of fire officers, the Korean version of the depression tool (PHQ-9; Patient Health Questionnaire-9) was conducted before and after the Stress Resilience Enhancement Program. The PHQ-9 was developed by Spitzer et al. (1999) and translated into Korean by Choi et al. (2007), and its purpose was to detect mental diseases that are likely to be encountered in primary clinical scenes and help the diagnoses. Park et al. (2010) verified the tool’s reliability and validity, and it is comprised of total 9 items standardized by Ahn et al. (2013). The items are rated on a 4-point Likert scale: ‘Not at all (0 point)’, ‘Several days (1 point)’, ‘More than a week (2 points)’, and ‘Nearly every day (3 points)’. The scores range from 0 to 27, with higher scores indicating more severe depression. Cronbach’s α in this study was 0.92.
Mood states
To measure the mood states of fire officers, the Korean version of Profile of Mood States-Brief (K-POMS-B) was conducted before and after the Stress Resilience Enhancement Program. The K-POMS-B is a self-report survey measuring the mood changes affected by the environment and human relations, comprised of total 30 items developed by Mcnair et al. (1971) and adapted in Korean by Yeun and Shin-Park (2006). The items are rated on a 5-point Likert scale: ‘Not at all (0 point)’, ‘A little (1 point)’, ‘Moderately (2 points)’, ‘Quite a Lot (3 points)’. And ‘Extremely (4 points)’. Lower scores indicate better mood states. The subfactors are comprised of tension, fatigue, anger, confusion, depression, and vigor. Total mood states are measured with the total mood disturbance (TMD) scores obtained by subtracting the vigor score from the sum of the five subfactors’ scores. Cronbach’s α was 0.63–0.96 at the point of the tool development, and Cronbach’s α in this study was 0.87–0.89.
Forest therapy program
The forest therapy program implemented in this study is the Stress Resilience Enhancement Program comprised of various contents for 5 days and 4 nights. It is a customized program developed for fire officers to overcome the trauma from PTSD by experiencing various elements of the forest away from everyday life and enhance stress resilience by cultivating the ability to manage their biorhythms. The program was carried out for 22 hours in total 5 days and 4 nights, and the detailed contents and schedules are as shown in Table 1. There were 9 hours of outdoor activities to feel the spirits of the forest using various environmental factors such as forest walking and meditation; 9 hours of indoor activities such as hydrotherapy, tea meditation, sound meditation, and aromatherapy; and 4 hours of special lectures on mental health by psychology lecturers from the outside.
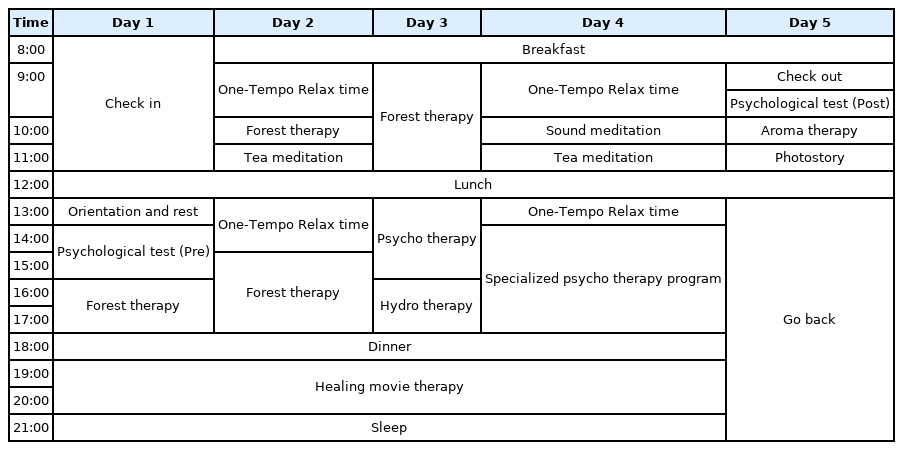
Contents of Stress Resilience Enhancement Program
Data analysis
A self-report questionnaire was developed using the aforementioned tools. The survey was conducted after providing sufficient explanation and introduction indoors. The fire officers participated in the survey twice: during orientation before the program and during the wrap-up time after the program. Data collected in this study were survey responses of 268 fire officers who participated in the Stress Resilience Enhancement Program, and the data of 185 participants excluding nonresponses and insincere responses were ultimately used in analysis. Frequency analysis was conducted to identify the demographic characteristics of the participants, and Wilcoxon signed-rank test to examine the differences in PTSD, depression, and mood states depending on the demographic characteristics before and after the program. Statistical analysis was conducted using SPSS ver. 24.0 (IBM Corp., USA), and the significance level was p < .05.
Results and Discussion
Demographic characteristics
The demographic characteristics of 185 fire officers participating in this study are comprised of gender, age, smoking status, average hours of sleep, drinking frequency, exercise frequency, job, rank, and period of service, and the response items are comprised of forest visit frequency and time spent in the forest (Table 2). As a result of analysis, there were 176 male (95.1%) and 9 female participants (4.9%), showing that most were male fire officers. Most of them were in their 30s (62, 33.5%), followed by 40s (53, 28.6%), 50s (46, 24.9%), 20s (20, 10.8%), and 60s and above (4, 2.2%). There were more non-smokers (135, 73.0%) than smokers (50, 27.0%) and most of them (71, 38.4%) slept 6 hours on average. Most drank once a week (60, 32.4%) and exercised 2–3 times a week (89, 48.1%).

General characteristics of subjects
By job, more than half of the participants (107, 57.8%) were in charge of fire investigation, followed by rescue/first aid (54, 29.2%) and public administration (19, 10.3%). By rank, most were firefighters (54, 29.2%), followed by fire captains (49, 26.5%), fire engineers (40, 21.6%), fire lieutenants (35, 18.9%), fire marshals (6, 3.2%), and fire battalion chief (1, 0.5%), showing that fire officers in various ranks participated in the study. Most of them worked for less than 10 years (107, 57.8%), followed by 10–20 years (41, 22.2%) and 20–30 years (35, 18.9%).
For forest visit frequency, most of the participants visited the forest 1–2 times a month (64, 34.6%), followed by 1–2 times a year (60, 32.4%). Most spent 30 minutes to 1 hour in the forest (70, 37.8%), followed by 1–3 hours (67, 36.3%), less than 30 minutes (38, 20.5%), and more than 3 hours (10, 5.4%) (Table 3).

Response items about forest
Analysis results of PTSD
As a result of analyzing the PTSD scores of fire officers participating in the Stress Resilience Enhancement Program (Table 4), the mean decreased from 10.65 (± 2.00) to 5.64 (± 8.29) after the program, showing a statistically significant difference (p < .001).

Results of post-traumatic stress disorder (PTSD) before and after the forest therapy program
The analysis results of PTSD scores of fire officers depending on demographic characteristics are as shown in Table 5, and only the mean and standard deviation (SD) are provided for items with N less than 10. By gender, ‘male’ showed a decrease in PTSD scores with a statistically significant difference (p < .001) after participating in the program. By age, there was a significant decrease (p < .001) in all of ‘20s’, ‘30s’, ‘40s’, and ‘50s’ except ‘60s and above (n = 4)’. By smoking status, both ‘smokers’ and ‘non-smokers’ showed a significant decrease (p < .001). By average hours of sleep, fire officers sleeping for ‘5 hours or less’, ‘6 hours’, and ‘7 hours’ (p < .001) and fire officers sleeping for ‘8 hours’ (p < .01) both showed a significant decrease, except those sleeping for ‘9 hours or more (n = 2). By drinking frequency, there was a significant decrease among all fire officers except ‘more than 4 times a week (n = 5)’, such as ‘not drinking’, ‘once a week’, ‘2–3 times a week’, and ‘1–3 times a month’ (p < .001). By exercise frequency, there was a statistically significant decrease among all fire officers except ‘no exercise (n = 4)’ and ‘1–3 times a month (n = 4)’, such as ‘once a week’ (p < .01) and ‘2–3 times a week’, ‘more than 4 times a week’ (p < .001). By job, there was a significant difference in ‘fire investigation’, ‘rescue/first aid’ (p < .001), and ‘public administration’ (p < .05). By rank, there was a statistically significant difference in all ranks such as ‘firefighter’, ‘fire engineer’, ‘fire lieutenant’, and ‘fire captain’ (p < .001) except ‘fire marshal (n = 6)’ and ‘fire battalion chief (n = 1)’. By period of service, all showed a significant decrease (p < .001) such as ‘less than 10 years’, ‘10–20 years’, and ‘20–30 years’ except ‘more than 30 years (n = 2)’.

Results of post-traumatic stress disorder (PTSD) before and after the forest therapy program by general characteristics
As a result of analyzing PTSD scores for forest-related items, there was a statistically significant decrease in fire officers visiting the forest ‘1–2 times a week’, ‘1–2 times a month’, and ‘1–2 times a year’ (p < .001), and fire officers spending ‘less than 30 minutes’, ‘30 minutes–1 hour’, and ‘1–3 hours’ in the forest (p < .001).
Analysis results of depression
As a result of analyzing the depression scores of fire officers participating in the Stress Resilience Enhancement Program (Table 6), the mean decreased by 1.00 points from 3.21 (± 4.00) to 2.21 (± 3.47) after the program, showing a statistically significant difference (p l< .001).
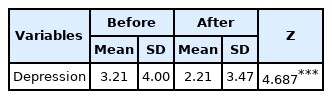
Results of depression before and after the forest therapy program
The analysis results of depression scores of fire officers depending on demographic characteristics are as shown in Table 7, and only the mean and SD are provided for items with n less than 10. By gender, ‘male’ showed a statistically significant decrease in depression scores after participating in the program (p < .001). By age, there was a significant decrease in ‘40s’ and ‘50s’ (p < .01). By smoking status, both ‘smokers (p < .05)’ and ‘non-smokers (p < .001)’ showed a significant decrease. By average hours of sleep, all fire officers showed a significantly decreased except those sleeping ‘7 hours’, such as ‘5 hours or less (p < .05)’, ‘6 hours (p < .001)’, and ‘8 hours (p < .01)’. By drinking frequency, there was a significant decrease in fire officers ‘not drinking’ (p < .05) and those drinking ‘once a week’ and ‘1–3 times a month’ (p < .001). By exercise frequency, there was a significant decrease in fire officers exercising ‘once a week’ and ‘more than 4 times a week’ (p < .05), and exercising ‘2–3 times a week’ (p < .001). By job, ‘fire investigation (p < .001)’ and ‘public administration (p < .05)’ showed a significant decrease, and by rank, ‘firefighter (p < .01)’, ‘fire lieutenant (p < .05)’, and ‘fire captain (p < .05)’ showed a significant decrease. By period of service, all fire officers showed a significant decrease in ‘less than 10 years’ and ‘10–20 years’ (p < .01), as well as ‘20–30 years’ (p < .05), except ‘more than 30 years (n = 2)’.

Results of depression before and after the forest therapy program by general characteristics
As a result of analyzing depression scores for forest-related items, there was a significant decrease in all fire officers except those visiting the forest ‘every day (n = 3)’, such as visiting ‘1–2 times a week’ (p < .05), ‘1–2 times a month’, and ‘1–2 times a year’ (p < .01). For time spent in the forest, there was a significant decrease in fire officers spending ‘30 minutes–1 hour’ (p < .05) and ‘1–3 hours’ (p < .001) in the forest.
Analysis results of mood states
As a result of analyzing the mood state scores of fire officers participating in the Stress Resilience Enhancement Program (Table 8), the means of subfactors of negative mood states such as tension, fatigue, anger, confusion, and depression decreased after participating in the program, showing a statistically significant difference (p < .001). Vigor, which is a subfactor representing a positive mood state, increased with a statistically significant difference after the program (p < .001). TMD representing the total mood states also decreased by 13.16 points after the program from 5.78 (± 17.37) to −7.38 (± 10.35), showing a statistically significant difference (p < .001).
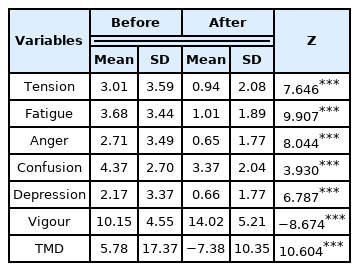
Results of profile of mood states (POMS) before and after the forest therapy program
The analysis results of mood state scores of fire officers depending on demographic characteristics are as shown in Table 9, and only the mean and SD are provided for items with n less than 10. By gender, ‘male’ showed a statistically significant decrease in mood state scores after the program (p < .001), and by age, all except ‘60s and above (n = 4)’ decreased significantly, such as ‘20s’, ‘30s’, ‘40s’, and ‘50s’ (p < .001). By smoking status, both ‘smokers’ and ‘non-smokers’ showed a significant decrease (p < .001). By average hours of sleep, fire officers sleeping for ‘5 hours or less’ (p < .01), ‘6 hours’, ‘7 hours’, and ‘8 hours’ (p < .001) all showed a significant decrease. By drinking frequency, all fire officers (p < .001) except those drinking ‘more than 4 times a week (n = 5)’, such as ‘not drinking’ or drinking ‘once a week’, ‘2–3 times a week’, and ‘1–3 times a month’ showed a significant decrease. By exercise frequency, all (p < .001) except those ‘not exercising (n = 4)’ and exercising ‘1–3 times a month (n = 4)’, such as ‘once a week’, ‘2–3 times a week’, and ‘more than 4 times a week’ showed a statistically significant difference. By job, there was a significant difference in ‘fire investigation’, ‘rescue/first aid’, and ‘public administration’ (p < .001). By rank, all ranks (p < .001) except ‘fire marshal (n = 6)’ and ‘fire battalion chief (n = 1)’, such as ‘firefighter’, ‘fire engineer’, ‘fire lieutenant’, and ‘fire captain’ showed a statistically significant difference. By period of service, all (p < .001) showed a significant decrease except ‘more than 30 years (n = 2)’, such as ‘less than 10 years’, ‘10–20 years’, and ‘20–30 years’.
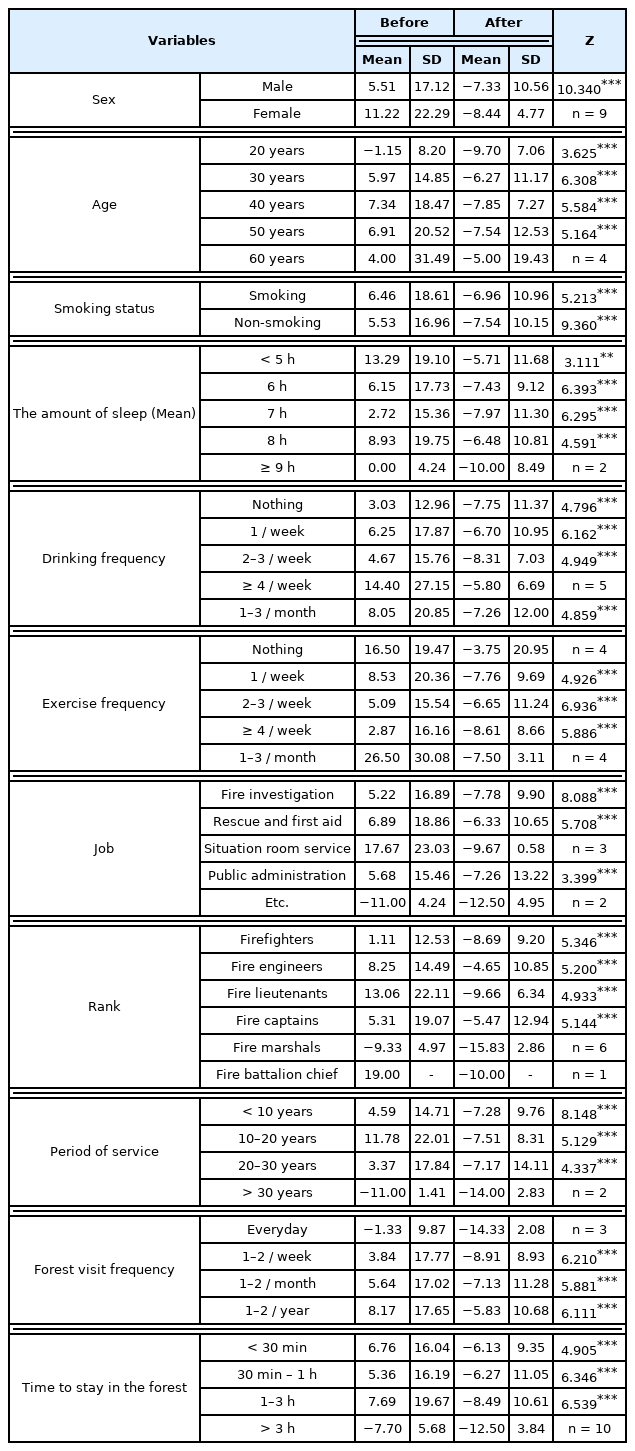
Results of profile of mood states (POMS) before and after the forest therapy program by general characteristics
As a result of analyzing mood state scores for forest-related items, there was a statistically significant decrease in fire officers visiting the forest ‘1–2 times a week’, ‘1–2 times a month’, and ‘1–2 times a year’ (p < .001), and fire officers spending ‘less than 30 minutes’, ‘30 minutes–1 hour’, and ‘1–3 hours’ in the forest (p < .001).
Conclusion
This study was conducted to determine the effect of forest therapy programs on PTSD, depression, and mood states of fire officers exhausted both physically and mentally from PTSD caused by working at urgent and terrible scenes of accidents as well as irregular working hours with overtime work and shifts.
As a result of analyzing the psychological scales from the survey before and after participating in the forest therapy program, there was a decrease in PTSD and depression and an increase in mood states. This is consistent with the results that forest therapy programs reduce PTSD of fire officers and improve mood states (Park et al., 2019). This also supports the results of previous studies that programs in recreational forests reduce stress of fire officers (Shin et al., 2018), and aromatherapy, forest therapy, and meditation programs have a positive effect on the mental health of fire officers (Jo, 2014).
As a result of comparatively analyzing the results by demographic characteristics, 20s and 30s showed improvement in only PTSD and mood states, whereas 40s and 50s showed statistically significant improvement in PTSD, mood state, and depression after the program. 40s and 50s had higher depression levels before the program and showed a more significant decrease afterwards. Middle-aged people are affected by multiple factors such as basic livelihood, housing, and future preparedness deprivation in terms of depression levels compared to the youth (Yeo, 2020). With the recently decreasing job security in the COVID-19 pandemic, it is becoming more important and urgent to establish institutional measures to reduce depression for middle-aged fire officers that are vulnerable to danger and heavy workload. PTSD and mood states decreased with a statistically significant difference in all jobs, and depression showed a significant difference in jobs except rescue/first aid, such as fire investigation and public administration. There was no statistical significance due to the small number of participants (n = 3), but fire officers working in the situation room especially showed higher TMD in mood states compared to other jobs before the program and ended up showing a significant improvement after the program. This implies that fire officers working in the situation room are vulnerable to greater mental damages and mood disorders than other jobs due to stress from urgent and tense states in an indoor environment for a long time. It is necessary to conduct research on the effects of forest therapy programs on more fire officers working in situation rooms.
For forest-related items, PTSD and mood states improved with a significant difference in all items. There was no statistically significant difference in depression for fire officers spending ‘less than 30 minutes’ in the forest, whereas there was a statistically significant difference for fire officers spending ‘30 minutes–1 hour’ and ‘1–3 hours’. In particular, one thing commonly found in all three indicators of PTSD, mood states, and depression depending on the time spent in the forest was that fire officers spending longer time in the forest showed higher explanatory power of the improvement results. This indicates that those visiting the forest and spending more time (1–3 hours) obtain more effect from the forest therapy program. A previous study examined the physiological effect of the forest depending on the time spent and discovered that there was a high frequency of the recovery effect when spending 2–4 hours in the forest (Jeong and Ahn, 2012). However, there must be an additional study on whether experience based on time spent in the forest in everyday life actually has a psychological and physiological effect.
This study has significance in verifying that forest therapy programs can be used as a method to recover and support physical and mental health of fire officers and providing scientific grounds based on collected data. Further research must be conducted to use as basic data to reduce PTSD and enhance mental resilience of fire officers through forest therapy programs and also establish systematic management plans for their mental and physical health. The scope of research should also be expanded to various other groups suffering from PTSD, such as the police and military, as well as medical workers and victims of the recent COVID-19 pandemic, so that they can find psychological and physiological recovery and stability through forest therapy programs.
Notes
This study was studied with the support of cooperative projects of Korea Forest Welfare Institute and National Fire Agency in 2019.