Mood State Changes in Patients with Metabolic Syndrome in the Urban Forests
Article information
Abstract
This study aims to assess forest healing programs to middle-aged people in Korea with metabolic syndrome as a method to control the syndrome through prevention and health improvement rather than treatment. In order to develop healing programs in the urban forests for metabolic syndrome patients, environment condition of the forests and moods of participants were compared. Thermal environments and the concentration of phytoncides were analyzed by the site. Saneum Healing Forest had a lower temperature but a higher humidity than Seoul Forest. Seoul Forest had higher PMV and PPD levels than Saneum Healing Forest, providing patients with freshness. This seems to be due to the seasonal factor of autumn. As for the total emissions of phytoncide, mountain forest generated more than urban forest. Nine components out of investigated twenty turned out to be generated more in the urban forests. The atmospheric composition of phytoncides, volatile organic compounds that are released from vegetation, was analyzed at both sites. Profile of Mood States (POMS) was measured before and after the healing program. The POMS suggested that forest environments reduce stress and increase comfort, calm, and feelings of refreshment. The tendency towards positive mood state in the forest recommend that middle-aged Metabolic syndrome patients participate in healing programs in the forests.
Ⅰ. Introduction
Korean people mostly want to spend leisure time on selfdevelopment or doing outdoor activities such as traveling and watching art and cultural performances, but in reality, they spend leisure time on doing indoor activities mostly such as watching TV or surfing the web (Ministry of Culture Sports Tourism, 2014). Even though recently walking is popular, the ratio of males who did walking exercise over ten minutes for one time within the last week significantly dropped from 62.4% in 2005 to 41.7% in 2013, and that of females also declined from 59.0% to 34.4%. Metabolic syndrome is a cluster of metabolic abnormalities associated with an increased risk of developing cardiovascular diseases or type II diabetes. The etiology of metabolic syndrome is not still unknown but complex. Over the same period, however, the prevalence rates of hypertension, diabetes and dyslipidemia were on the rise (Ministry of Health and Welfare and Centers for Disease Control & Prevention, 2014), and the number of patients treated for metabolic syndrome as of 2014 reached 9.91 million (Health Insurance Review & Assessment Service, 2015), which makes it difficult to say that they are irrelevant. This is attributable to the fact that the improvement of lifestyle habits is crucial to the occurrence and prevention of metabolic syndrome, and particularly that it is most important to reduce weight and body fat through weight losses, regular exercises and improved eating habits (Den Boer et al., 2013; Fappa et al., 2008; Hellenius, 2008).
The reasons why metabolic syndrome should be paid attention are, though controversial, that patients with metabolic syndrome have higher risks of cardiovascular diseases and type 2 diabetes (Kim and Park, 2012; Pirjo and Jaakko, 2013; Wilson et al., 2005), and that the burden of medical expenses due to chronic diseases has continued to increase. Meanwhile, it was reported that three out of four people in Seoul had risk factors for metabolic syndrome, and, in particular, males in their 40s and 50s and post-menopausal females were found to have metabolic syndrome (Hanm, 2011; Metabolic Syndrome Management Center of Seoul, 2009). Metabolic syndrome develops slowly and it takes a long time for it to develop into a disease. Against this backdrop, for those who are exposed to risk factors for it, the central and local governments have been implementing metabolic syndrome management programs for prevention and health improvement because they are as important as treatment (Ministry of Health and Welfare, 2013; Seoul, 2014).
Although the majority of people living in urban areas face health risks due to metabolic syndrome, it is still worthwhile to adopt approaches in living environments if they can be prevented by improving lifestyle habits. Early studies on patients with metabolic syndrome focused on physiological effects of intervention through exercises and improved diet (Oak, 2015). According to the experiment in Beijing, Chronic exposure to air pollution particles increases the risk of obesity and metabolic syndrome (Wei et al., 2016). Those on the effects of forest healing utilizing the physical elements of forest environment also mainly focused on the stress relieving in healing forests and recreational forests outside urban areas targeting ordinary people in their 20s (Choi, 2015). As healing programs to verify forest’s health improvement and healing effects have been attempted, the target groups of such studies have expanded into patients with asthma, atopy, hypertension and diabetes, and even alcoholics and schizophrenic patients (Lee, 2014; Ohtsuka et al., 1998; Yoo et al., 2011). Forest healing program positively affected the mood state of employees with work-related stress and cancer patients (Kim, 2015; Lee, 2015), changes of the mood state was also beome better by the wood essential oil (Song et al., 2014), and the mood states depend on the tree species in the forest (Jeong, 2016). A recent study on patients with metabolic syndrome focused on recreational forests (Jeong, 2016), but there is no study focusing on urban forests. Against this backdrop, this study aimed to apply forest healing programs to patients with metabolic syndrome that have been attempted since the 1978 Alma-Ata Declaration having called for the transition from treatment-oriented healthcare polices to those centered on prevention and health improvement.
Since abdominal obesity, one of the diagnosis criteria for metabolic syndrome, is affected by depression and stress (Kiecolt-Glaser, 2015; Son and Kim, 2012), a forest healing program was conducted for patients with metabolic syndrome in urban forests. Changes in their mood state after the program were analyzed to verify the effectiveness of the program. The purpose of this study is to analyze changes in the mood state of patients with metabolic syndrome after using urban forests and atmospheric condition, and ultimately to provide useful basic information for the development of forest healing programs as a health improvement activity using urban forests that are highly accessible by patients with metabolic syndrome living in urban areas.
Since abdominal obesity, one of the diagnosis criteria for metabolic syndrome, is affected by depression and stress (Kiecolt-Glaser, 2015; Son and Kim, 2012), a forest healing program was conducted for patients with metabolic syndrome in urban forests. Changes in their mood state after the program were analyzed to verify the effectiveness of the program. The purpose of this study is to analyze changes in the mood state of patients with metabolic syndrome after using urban forests and atmospheric condition, and ultimately to provide useful basic information for the development of forest healing programs as a health improvement activity using urban forests that are highly accessible by patients with metabolic syndrome living in urban areas.
Ⅱ. Research methods
1. Research design
In this study, natural elements of urban forests were applied for the purpose of the development of a forest healing program for patients with metabolic syndrome. Since a forest healing program is to promote health through improved lifestyle habits, not to diagnose or treat it, psychological changes and physical environmental conditions were analyzed and mountain forests and urban forests were compared. Development of the forest healing programs consisted of exercise therapy, education, meditation and natural observation awakening the five senses based on analysis of characteristics of metabolic syndrome patients.
To demonstrate the effect of accessible urban forest use on the improvement of lifestyle habits of patients with metabolic syndrome, firstly, the atmospheric conditions and physical environments of urban forests and a mountain forests were measured and compared. Secondly, changes in the mood state of the patients before and after the urban forest healing program were evaluated and compared with changes in the mood state of the patients in the mountain forests.
2. Research participants and sampling method
This study was approved by the Institutional Review Board (IRB, IRB No. 15143). Among male and female adults in their 40s to 60s living in Seoul, those who were diagnosed with metabolic syndrome and registered by local public health centers were individually contacted via phone calls with the support of the Metabolic Syndrome Management Center of Seoul. They were informed of this study and research participants were recruited among those who applied for this program.
Metabolic syndrome is a cluster of abnormal conditions that raise risks for cerebrovascular and cardiovascular diseases and diabetes including excess body fat, increased blood pressure, high blood sugar and abnormal lipid levels. Metabolic syndrome criteria in Korea requires three of the five following cases (Ministry of Health and Welfare, 2015): ① when the waist circumferences of a male and a female are equal to or greater than 90 cm and 85 cm respectively, ② when neutral fat is equal to or greater than 150 mg/dL, ③ when the HDL cholesterol levels of a male and a female are less than 40 mg/dL and 50 mg/dL respectively, ④ when blood pressure is equal to or greater than 130/85 mmHg, and ⑤ when fasting glucose is equal to or greater than 100 mg/dL or those who have a diabetes history or have taken medicine. In this study, along with the five criteria above, applicants who have the following requirements were selected: ① voluntary participants, ② aged 40s-60s, and ③ stop smoking and drinking for a week prior to the participation in this program. Those who have any of the following conditions were excluded: ① those who regularly took substances (antioxidants or similar substances) that could affect the reactive oxygen species (ROS), ② those who were undergoing hormone replacement therapy, ③ those with alcohol syndrome, ④ those with cardiovascular diseases (cardiac insufficiency, using a cardiac pacemaker), ⑤ those with renal diseases (renal insufficiency, inflammation in urinary system), ⑥ those with liver diseases, especially hepatitis, ⑦ those who were a cancer patient as of the time of the program or had a cancer history. The final participants were informed orally of the purpose and procedure of this study and they signed the consent form for the participation in this program in their own handwriting.
3. Selection of research location and measurement of atmospheric conditions
Two locations-mountain forest and urban forest were selected to compare the effects of forest healing of different environments. The mountain forest selected in this study was Saneum Healing Forest located in Yangpyeong, the first designated national healing forest and the urban forest selected in this study was Seoul Forest which is located at the center of Seoul, and thus highly accessible.
Saneum Healing Forest is located in Danwol-myeon, Yangpyeong-gun, Gyeonggi-do, and is developed on an area of about 56 ha in a natural recreational forest with the area of 2,140 ha. It is developed at an altitude ranging from 270 m to 940 m. Its vegetation is comprised of Pinus koraiensis forest, Larix kaempferi forest, and mixed forests of broad leaves and narrow leaves. Saneum Healing Forest has different geographical features, and valleys. Seoul Forest is located in Seongsu-dong, Seongdong-gu, Seoul, and is developed on an area of 11.6 ha. There are high-rise mixed-use buildings with residential and industrial areas are constructed surrounding Seoul Forest. This flatland forest is divided into five sections including nature experiencing study field and ecological forest, and various species of ornamental plants are planted between small-scale Pinus densiflora forest, Pinus koraiensis forest, Ginko biloba forest. To compare differences in the environments of the two forests, data on key factors for forest healing, phytoncide, and thermal environment were collected and analyzed for the one and half hour program.
1) Thermal environment
A comfortable condition in a thermal environment means an environment where people do not have stress or feel discomfort. According to ISO 7730:2005, comfort is defined as a state of a mind in which people are satisfied with a thermal environment (ISO, 2015). To identify differences in thermal environments of Saneum Healing Forest and Seoul Forest, a portable multifunctional handheld measuring instrument (MI 6401 POLY, METREL, Slovenia) was used to measure temperature, humidity, wind speed, dew point, globe temperature, air velocity, and wet-bulb globe temperature every one minute. To reduce measurement error, the data collected five minutes before and after measurement were excluded and Predicted Mean Vote (PMV) and Predicted Percentage of Dissatisfied (PPD) were analyzed using SensorLink PRO software (METREL, Slovenia). The PMV is the concept developed by Fanger (1970), a Dane expert in the filed of thermal comfort and perception, and there are six subscales to take into consideration when analyzing thermal comfort including temperature, humidity, air velocity, radiant temperature, clothing insulation and metabolic rate. The thermal scale used in the PMV runs from-3 to 3, having seven values. When a score is closer to zero, people feel comfortable. When a score goes up in a positive direction, they feel hotter, and when it goes down in a negative direction, they feel colder. The PPD shows the percentage of participants who feel dissatisfied with a certain thermal environment (Table 1).

ANSI/ASHRAE Standard 55-2013: Seven point thermal sensation scale (ASHRAE, 2013).
2) Phytoncide
Phytoncides are Natural Volatile Organic Compounds (NVOCs) emitted by forests, mainly comprised of isoprene and terpene (Harrison et al., 2001). In this study, twenty-two NVOCs were measured at the three points of the each forest types, and among them, data on twenty compounds were collected.
To collect phytoncide samples, a Tenax TA absorbent tube filled with Carbotrap (Supelco, USA) was horizontally installed at the height of 1.5 m from the ground. The collected samples were analyzed using a Gas Chromatography/Mass Spectrometer (GC/MSD, 7890N-5975, Agilent, USA) equipped with an automatic thermal desorber (Gerstel TDS, Gerstel, Germany). Target compounds absorbed within the tube were thermally desorbed first at 280°C for six minutes within a trap desorber by injecting high-purity helium gas at the velocity of 50 ml/min. They were concentrated at -30°C at a cold trap, and after that, were thermally desorbed again at 300°C for three minutes and injected into the gas chromatography/mass spectrometer to analyze.
4. Measurement of mood state
Fifteen participants gathered at Saneum Healing Forest started the program at 9 am on October 7th in 2015 and the next day fourteen participants at Seoul Forest started the program at 9 am. All participants had a light meal before the program. A pre-test questionnaire survey was conducted to measure their mood state. After the program, a post-test questionnaire survey was also conducted to check any changes in their mood state. The translated version (Kim, 2001) of the Profile of Mood States (POMS) developed by McNair et al. (1971). was used in the surveys. The questionnaire is divided into seven sub-factors including tension, depression, anger, vigor, fatigue, confusion and friendliness, and has sixty-five questions in total with the 5-point scale (1=strongly disagree, 2=disagree, 3=neutral, 4=agree, 5=strongly agree). A higher score means a lower mood state in most questions, except one question on tension, one question on confusion, and eight questions on vigor. In the questions where a higher score means a higher mood state, the scores of the questions were reverse-coded to compare results consistently with others. The sixty-five questions were divided into nine questions on tension (45 scores), fifteen questions on depression (75 scores), twelve questions on anger (60 scores), eight questions on vigor (40 scores), seven questions on fatigue (35 scores), and seven questions on confusion (35 scores). Changes in the mood state of a participant before and after the program were analyzed by calculating the Total Mood Disturbance (TMD) and the average of the scores added by sub-factors. TMD scores were computed by adding the scores for tension, depression, anger, fatigue and confusion and then subtracting the score for vigor. According to Lee and Kim (2006), friendliness is more like a characteristic, not a mood state, and thus it has been excluded in other studies often. In this study, the results of fifty-eight questions excluding seven questions on friendliness were analyzed only.
With the valid data of the collected results, statistics analysis was performed using SPSS 18.0, and the significance level was 0.05. Assessment of the mood states yielded to check changes in the mood state and TMD of the participants and a paired t-test was conducted on the collected data through the pre-test and post-test surveys which contained 58 statements of each of the six subscales. The unpaired t-test was used to compare the differences between the mountain forest group and the urban forest group.
Ⅲ. Results and discussion
1. Analysis of thermal environment and phytoncide
The average temperatures of Saneum Healing Forest and Seoul Forest during the program were 18.26°C and 22.14°C respectively, showing a difference, about 4°C (Table 2). The relative humidity levels of Saneum Healing Forest and Seoul Forest were measured to be about 80% and 70% respectively, indicating that atmospheric conditions were different. Based on the results, the Predicted Mean Vote (PMV) was -0.91 in Saneum Healing Forest and 0.09 in Seoul Forest. When the value is closer to zero, it is interpreted that people have less stress and tension from thermal conditions. Thus, it was found that the participants felt more comfortable in Seoul Forest than in Saneum Healing Forest with a lower temperature. Likewise, the Predicted Percentage of Dissatisfied (PPD) was 27.72 in Saneum Healing Forest, over three times higher than the PPD (8.84) in Seoul Forest, which is attributable to the atmospheric conditions with lower temperature and higher relative humidity.

Comparison of atmospheric conditions and thermal comfort indices.
The precedent studies on the comparison of comfort in thermal environments were mostly conducted in comparing summer forest environments with urban environments, and they concluded that thermal comfort was higher in those with large scale green areas (Yoon et al., 2014). In this study, however, the program was conducted in autumn when the temperature starts to decline, and thus it was found that the participants felt more comfortable at a higher temperature than at a slightly lower temperature.
The total volume of phytoncides, natural volatile organic compounds emitted by forests, in Saneum Healing Forest, was 25.58 ng・m-3 , higher than that of Seoul Forest (18.44 ng・m-3 , Table 3). Out of the collected twenty compounds, the volumes of eleven compounds including α-pinene, camphene, and β -pinene were higher in Saneum Healing Forest than in Seoul Forest. The volumes of the rest nine compounds including limonene were higher in Seoul Forest than in Saneum Healing Forest. The volume of phytoncides is associated with a season, weather factors and time (Lee et al., 2011; Lee et al., 2012), and depending on the sizes of forests, the types of trees, and whether their spaces are encircled or open, the volume of phytoncides can vary. The sizes of forests are closely related to the volume of trees that emit phytoncides, and the openness of large-scale forests and urban parks has a negative correlation with the volume of volatile organic compounds that can be captured and the number of compounds.

Comparison of NVOCs concentration at one sampling point showing average, maximum, and minimum concentration in each site.
2. Changes in mood state
To identify the effects of the forest healing program conducted on the urban forest and the large-scale forest on the mood state of patients with metabolic syndrome, pre- and post-test questionnaire surveys were conducted on the mood state among the participants of the program both in Saneum Healing Forest and Seoul Forest. To check the homogeneity of the pre-program mood state of the two groups, a t-test was conducted and then homogeneity was achieved two of them. Total scores of POMS for each site were analyzed and the results are as follows (Table 4).
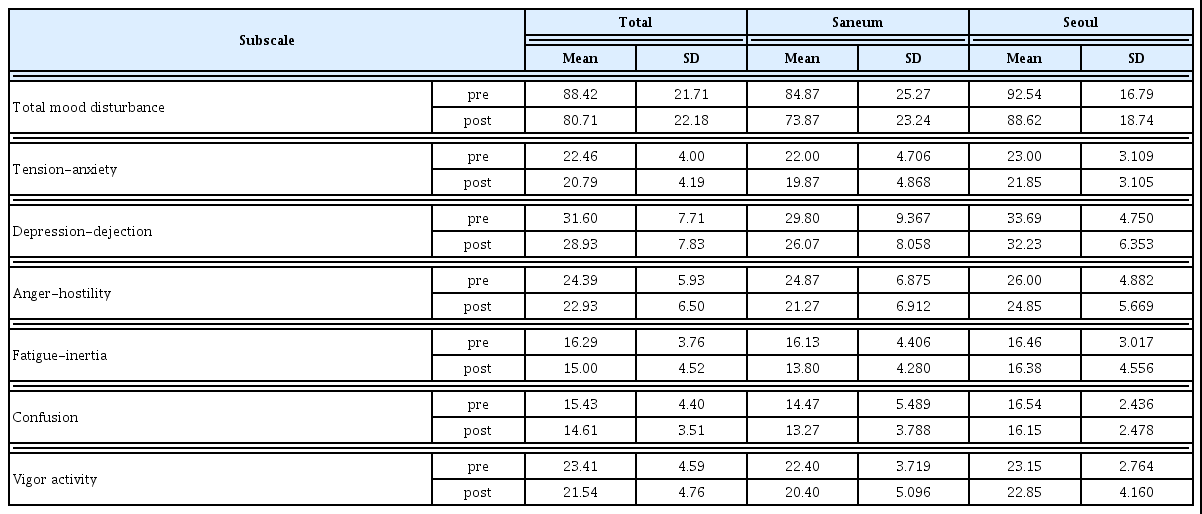
Pre-post (mean ± standard deviation) of each subscale of the POMS questionnaire.
Changes in the average scores and TMD scores before and after the program were analyzed by subscale (Table 5), and there was no statistically significant difference between Seoul Forest and Saneum Healing Forest. This indicates that the changes in the mood state of the two participant groups of Saneum Healing Forest and Seoul Forest were not different. In terms of subscale, the average score of tension in Seoul Forest declined from 23 (3.109) to 21.85 (3.105), and that in Saneum Healing Forest also decreased from 22 (4.706) to 19.87 (4.868). The average score of depression in Seoul Forest declined from 33.69 (4.750) to 32.23 (6.353), and that in Saneum Healing Forest also decreased from 29.80 (9.367) to 26.07 (8.058), but they all did not show any statistically significant difference. The average score of anger in Saneum Healing Forest decreased from 24.87 (6.875) to 21.27 (6.912), the only statistically significant decline, but that in Seoul Forest declined from 26 (4.882) to 24.85 (5.669) with no statistically significant decrease. In terms of vigor, both the forests did not show any significant changes. The score of fatigue in Seoul Forest slightly declined from 16.46 (3.017) to 16.38 (4.556), and that in Saneum Healing also decreased slightly from 14.47 (5.487) to 13.80 (4.280). The average score of confusion in Seoul Forest declined from 16.54 (2.436) to 16.15 (2.478), and that in Saneum Healing Forest decreased from 14.47 (5.487) to 13.27 (3.788), but they all did not show any statistically significant difference. Such the results by subscale with no statistically significant difference between the two groups indicate that following the finding of an early study (Park, 2010) about the effectiveness of forest healing programs in the mountain forests outside urban areas, those conducted in urban areas can also give similar effects (Lee et al., 2011).
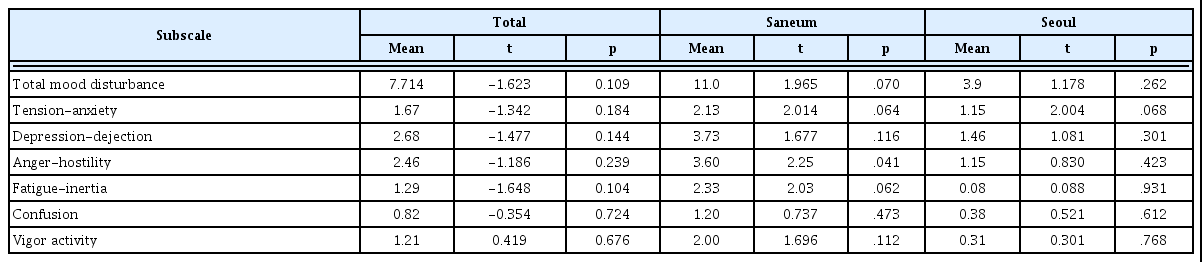
T-test statistics for POMS by forest type.
The limitation of this study is that of statistical or data limitation. Although the results of the forest healing program for patients with metabolic syndrome showed positive changes, but not statistically significant. In the study of Oak (2015) on the analysis of the frequency and period of intervention in patients with metabolic syndrome over the past five years, intervention was conducted three times per week for twelve weeks in over 50% of the analyzed cases, which indicates that the repeated implementation of such programs for a certain period can result in more effective analysis results. Instead of focusing on the discussion of the effects of the program, the results of this study can be used as useful basic information for follow-up studies to verify the effects of the urban forest healing program developed in this study for patients with metabolic syndrome.
Ⅳ. Conclusion
Metabolic syndrome is a cluster of abnormal metabolic conditions that raise risks for cardiovascular diseases and type 2 diabetes. The exact cause of metabolic syndrome has not been identified, but multiple personal and environmental factors were found to contribute to the rising risks of metabolic syndrome.
This study aims to apply forest healing programs to those who have been exposed to risk factors of metabolic syndrome, especially middle-aged people in Korea, as a method to control the syndrome through prevention and health improvement rather than treatment. Given the fact that most people in Korea live in urban areas, this study focused on a forest healing program using urban forests for patients with metabolic syndrome.
To develop an urban forest healing program for patients with metabolic syndrome, the results of early studies on the existing forest healing programs conducted on mountain forests were compared. The changes in the mood state of patients with metabolic syndrome before and after the forest healing program in the mountain forest and the urban forest were analyzed, and there was no significant difference between the two forests. Changes before and after the program were analyzed by dividing them into six different subscales (tension, depression, anger, vigor, fatigue and confusion). Statistically, significant differences were found only in the subscales of anger in the mountain forest, and except that, there was no statistically significant difference. However, it was found that all of the scores declined, indicating that the mood state of the patients improved in a positive direction.
In conclusion, the mood states of patients with metabolic syndrome in the urban forests were not bad by comparison with patients in the mountain forests, it is necessary to actively forest healing programs to improve the health of patients with metabolic syndrome in the urban forests.