A Needs Analysis for the Development of Forest Healing Programs: Focusing on Cancer Patients
Article information
Abstract
Background and objective
Cancer is the number one cause of death in Korea, and it affects any part of the body regardless of gender and age. Forest healing is a treatment that maximizes the effect of treatment and improves the quality of life. This study aims to provide basic data for the development and implementation of differentiated forest healing programs for cancer patients based on the survey on their interest and needs for the programs.
Methods
The subjects were those diagnosed with cancer from October 2018 to April 2019, and this study used 144 copies of the questionnaire retrieved. The sample size of this study (n = 144) was the appropriate size required by G-Power, and the collected responses were analyzed using SPSS 25.0.
Results
In the frequency analysis on the interest in forest healing, 79.2% of the subjects had no experience participating in forest healing, but 87% were aware of it, and 82.6% showed the intention to participate in forest healing programs. This indicates that even though not many of them have experience participating in forest healing, they showed high interest and needs for participation. They preferred to participate in spring (29.9%) and fall (27.8%), in programs carried out for 1.5–2 hours in the morning on weekdays.
Conclusion
This study has implications for the analysis on forest healing needs of cancer patients, and it is necessary to plan, develop, and implement differentiated forest healing programs that meet the needs of the cancer patients depending on their characteristics. There is also a need to plan forest healing program that can promote both psychological stability and physical health of cancer patients and verify and evaluate their effects based on specialized training of forest healing instructors.
Introduction
People today show greater interest in promoting health and preventing diseases, and the development of medical technology has led to the longer average lifespan. Nonetheless, stress, cerebrovascular diseases, neurosis, anxiety, depression, suicide, heart diseases, and cancer patients are increasing, and cancer is the number one cause of death in Korea. According to the 2018 statistics of National Cancer Information Center, total 79,153 deaths were caused by cancer, most of which were by lung cancer (22.5%, 17,852 deaths), followed by liver cancer (13.4%), colorectal cancer (11.1%), gastric cancer (9.8%), and pancreatic cancer (7.6%). By gender and mortality rates of major cancer types, 48,898 men died from cancer, indicating that 30.3% of all deaths in men are caused by cancer. Cancer with highest mortality rate in men was lung cancer (27%, 13,188 deaths), followed by liver cancer (15.9%), gastric cancer (10.4%), and colorectal cancer (10.1%). Total 30,255 women died from cancer, indicating that 22.0% of all deaths in women are caused by cancer. Cancer with highest mortality rate in women was lung cancer (15.4%, 4,664 deaths), followed by colorectal cancer (12.8%), pancreatic cancer (9.4%), and liver cancer (9.3%) (National Cancer Information Center, 2019).
Industrialization and urbanization increased people’s interest in recreation as well as desires for stability and recovery of health the mind and the body, which led to growing interest in forests for health and precaution against diseases. Forests began to be perceived as a place for relaxation and healing in the Forestry Culture and Recreation Act amended in March 2010. According to Article 2, paragraph (4) of this Act, forest healing is defined as ‘immune-strengthening and health-promoting activities, which utilize a variety of elements of the forest, including scents and scenic views’ (Korea Forest Service, 2011). As an intervention for treatment and recovery of cancer patients, there is an increasing need for a customized forest healing program based on target analysis in the planning process using natural ingredients of forests (Hong et al., 2010). Forests and natural materials are known to have a positive impact on emotional, psychological, and physical stability as well as self-realization and to alleviate depression, and thus used to treat, recover, and alleviate diseases such as cancer (Shin et al., 2007). Forest activities may be a physiological and psychological treatment as they reduce stress and increase alpha waves, and also affect the immune function (Park, 2010). In the attention restoration theory, forests help recover health physiologically and psychologically through being away, extent, fascination, compatibility, and comfort (Kaplan, 1995). Forest healing programs for subjects visiting the forest require a needs analysis according to the frequency of forest visits and a preference analysis according to the level of stress (Lee and Kim, 2011). A forest healing program that meets the characteristics and therapeutic goals must be developed depending on the subjects (Kim et al., 2014a). For the analysis of needs and preferences of the subjects, it is necessary to determine the theme, therapy, and accurate subject information (Kim, 2016b), and to develop a differentiated and customized program based on the disease through analysis of activities (Son et al., 2012). To maximize the therapeutic effects, activities must be carried out in forests with abundant physiological conditions (air, water, sunlight, anion, place, exercise, herbs, terpene) and mental conditions (Morita therapy, Zazen, behavior, music, amusement, kinesitherapy, autogenic training, forest smells, sounds of birds, winds, anion) (Kim, 2006). As such, previous studies had emphasized the need to develop a differentiated and customized program with preference and needs analyses according to the subjects visiting the forest. However, it is difficult to find research cases that analyzed the preference and needs for forest healing programs targeting cancer patients using the healing elements of the forest. Accordingly, this study was conducted to provide basic data for development and implementation of a differentiated forest healing program through surveys and analysis on interests and needs for forest healing with potential cancer patients that will be participating in the forest healing program.
Research Methods
Subjects and survey method
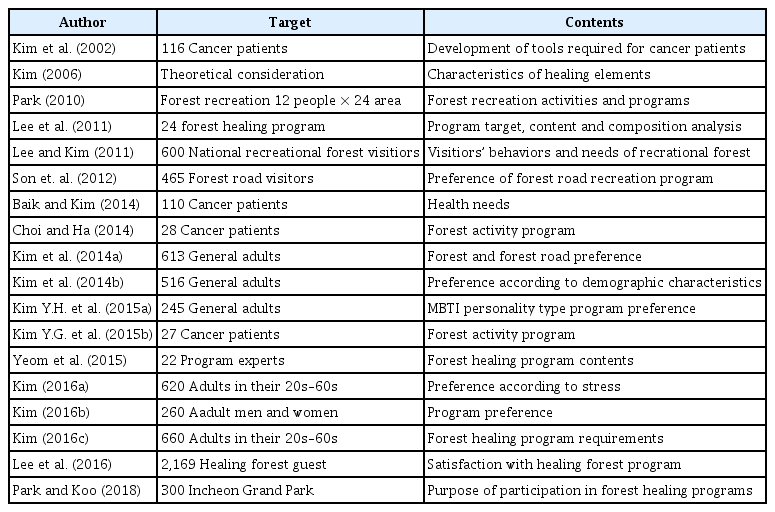
To develop the survey items that meet the purpose of this study, we analyzed 18 previous studies and came up with total 60 items: 6 demographic questions to determine the subjects, 9 questions on interest in forest healing. 6 questions on preference in forest healing programs (psychotherapy, kinesiology, climate therapy, plant therapy, water therapy, diet therapy), 25 sub-items, 4 questions on preference in the purpose of participating in a forest healing program (physical/psychological/social/cognitive), and 16 sub-items, with the preference and purpose developed to be rated on a five-point Likert scale (Table 1). To improve completeness of the questionnaire, five related experts (two Forest Therapist-Grade 1, forest education specialist, nurse, Horticultural Therapist Registered for Wellbeing-Grade I) developed and reviewed the questionnaire. Hospitalized cancer patients were excluded from the subjects due to the nature of this study. The subjects were recruited through cancer patients’ self-help groups and health centers in some parts of Gyeonggi-do, Gwangju (Jeonnam), Jinju (Gyeongnam), Jeju-do, Yesan and Seosan (Chungnam), and Cheongju (Chungbuk), among those diagnosed with cancer from October 2018 to April 2019. After explaining the intent and purpose of this study, we retrieved the self-administered survey from those who wanted voluntary participation and gave them serial numbers. Total 162 copies of the questionnaire were retrieved, but we used 144 copies for statistical analysis excluding 18 copies that lack accuracy and statistics.
Analysis of previous studies
Methods of data analysis
The survey responses were analyzed using SPSS 25.0. We used frequency analysis on the demographic characteristics and questions about interest in forest healing, descriptive statistics on preference in forest healing programs and purpose of forest healing to verify the expected outcomes of participation, chi-squared test and Fisher’s exact test to verify the differences of interest in forest healing depending on gender and name of the disease, and independent samples t-test and one-way ANOVA on preference in forest healing programs and purpose of the programs to verify the difference in preference.
Results and Discussion
Demographic characteristics of the subjects
The demographic characteristics of the subjects were analyzed by gender, age, marital status, occupation, and education. 30.6% were men (44 subjects) and 69.4% were women (100 subjects), most of which were in their 50s, and the female participation rate was higher since it was difficult to retrieve the survey from the male participants. 84% of them were married (121 subjects), and most of them were full-time homemakers (37.5%, 54 subjects), followed by professional practice, service, teaching/office, and production. Most of them were high school graduates (45.8%, 66 subjects), followed by middle school graduates, university graduates or higher, and elementary school graduates. 7. 7% of the subjects were under the age of 39 (11 subjects) and 13.2% were over 70 (19 subjects), and they had a variety of occupations (Table 2).

Demographic characteristics of the research subject
Clinical characteristics of the subjects
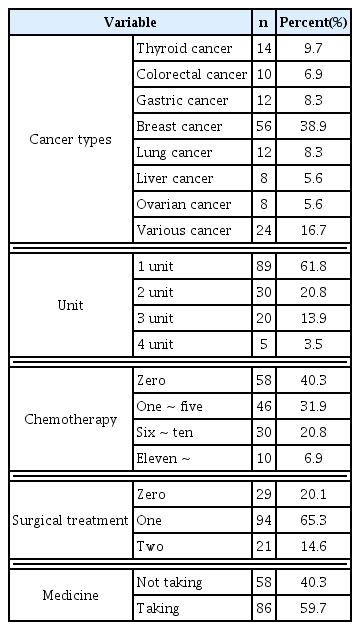
The subjects received treatment from minimum 1 month to maximum 5 years, for 10 months on average. Most had breast cancer (38.9%, 56 subjects) -- partly because there were more female subjects in this study -- followed by gastric cancer (38.9%) and lung cancer (38.9%), and 4 out of 14 subjects with thyroid cancer (9.7%) were men. 59.7% received chemotherapy, most of them were in Stage 1 (61.8%), and all subjects except 29 of them had already received surgical treatment at least once (Table 3).
Clinical characteristics of the study subject
Interest in forest healing
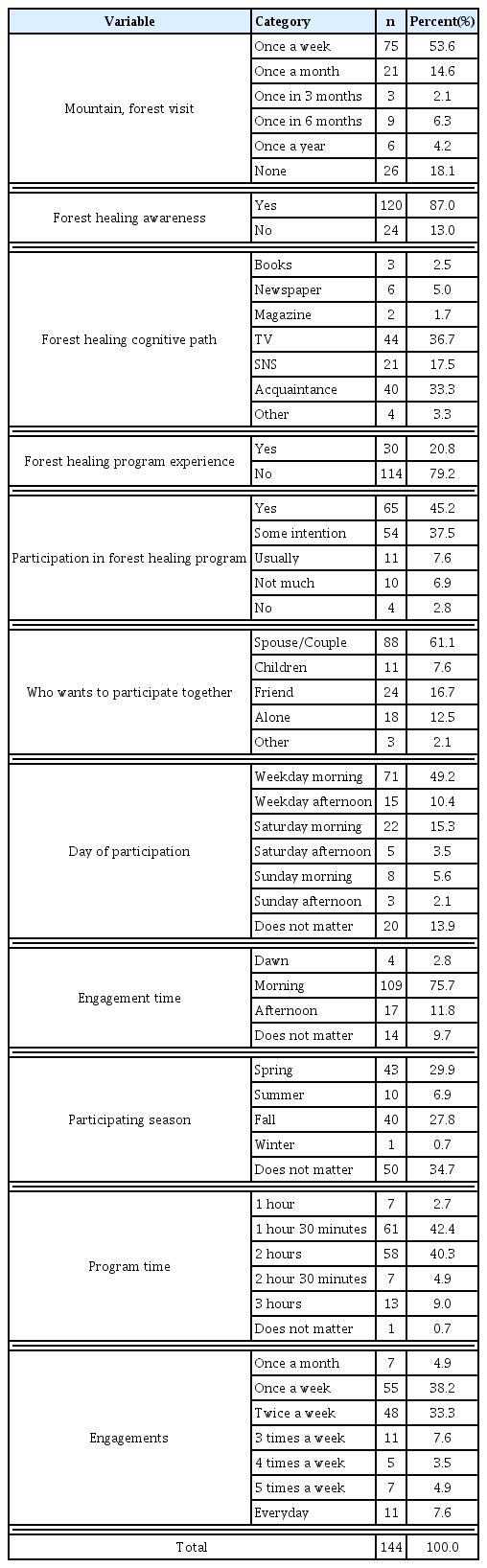
Multiple-choice questions were used to determine the interest in forest healing among the subjects. 52.1% (75 subjects) went to a mountain or a forest once a week, 14.6% (21 subjects) went once a month, 2.1% (3 subjects) went once every 3 months, 6.3% (9 subjects) went once every 6 months, 4.2% (6 subjects) went once a year, and 18.1% (26 subjects) almost never went. 87% (120 subjects) claimed to have heard of forest healing, 36.7% (44 subjects) on TV, 33.3% (40 subjects) on the internet, and 17.5% (21 subjects) on SNS, but 79.2% (114 subjects) had no experience participating in forest healing. 82.6% (118 subjects) were willing to participate in a forest healing program, and 9,8% (14 subjects) were not. In a previous study that surveyed the preference of adults in forest healing programs, men were more aware of forest healing than women, and most of whom experienced the programs were in their 50s, followed by 40s, 30s, and 20s (Kim et al., 2014b). 29.9% (43 subjects) responded they preferred spring, 6.9% summer (10 subjects), 27.8% fall (40 subjects), 0.7% winter (1 subjects), and 34.7% responded that the season does not matter (50 subjects). In a previous study, the 20s preferred half a day and a day, and 30s–50s preferred overnight and half a day (Kim et al., 2014b), but in this study, 42.4% (61 subjects) preferred 1 hour and 30 minutes, 40.3% (58 subjects) preferred 2 hours, and 9.0% (13 subjects) preferred 3 hours. 4.9% (7 subjects) said they want to participate once a month, 38.2% (55 subjects) once a week, 33.3% (48 subjects) twice a week, 7.6% (11 subjects) 3 times a week, 3.5% (5 subjects) 4 times a week, 4.9% (7 subjects) 5 times a week, and 7. 6% (11 subjects) every day (Table 4). An analysis on the visitor characteristics of healing forests showed that many visitors are satisfied with 2–4 hours of experience-based programs in the spring, but it is necessary to organize different programs depending on the disease (Kim et al., 2016b). Since satisfaction varies depending on whether one has a disease or not, the needs of the subjects must be reflected in order to create a good program (Lee et al., 2016). Thus, it is necessary to plan and develop specialized programs based on analysis of interests and needs of the subjects in forest healing and train forest therapists with professional knowledge in the programs. In this study, cancer patients had a high level of awareness about forest healing but had relatively little experience in actually participating in a forest healing program, and yet they showed a strong will to participate. Thus, there is a need for forest healing programs that are suitable for the characteristics of cancer patients by determining their needs and preferences to alleviate their psychological depression, anxiety, and stress and promote quality of life and physical functions. In addition, it is necessary to develop forest healing programs that meet the needs of the subjects according to the four seasons as well as the purpose and characteristics of the program and implement them in the actual scene based on effectiveness studies.
Forest healing interest
Difference of interest in forest healing depending on gender and cancer types
Difference of interest in forest healing depending on gender
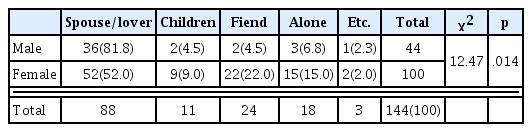
Interest in forest healing (who they want to participate with, number of visits, awareness of forest healing, path of forest healing awareness, intention to participate, desired day of the week, participating time, number of participations, season, gender) showed a significant difference depending on gender. More specifically, most men responded they want to participate with their spouse or lover (81.8%), whereas only 52% of women (52 subjects) responded the same, which showed a significant difference; other than that, there was no significant difference in the items of interest in forest healing (Table 5). In the needs for programs using urban forests, the 20s and 40s highly appreciated forest healing factors, while the 30s and 50s attached greatest importance to forest healing programs, claiming that differentiated programs must be provided depending on the age of participants (Park and Koo, 2018). A previous study stated that by gender, women preferred spring and men preferred fall, and by age, the 20s–30s preferred fall and the 40s–50s preferred spring; and since the sensitivity and emotions of the subjects all vary, the programs cannot be limited to just one season and instead must be differentiated by seasons (Kim et al., 2014b). As such, this study discovered that more women visited the forest than men and also more often, and that the subjects wanted to participate in the programs with their spouses or lovers. Thus, it is necessary to develop a program in which the subjects can participate with their spouses. There was a difficulty in securing the subjects due to the nature of their characteristics, but it seems necessary to conduct a systematic survey on the subjects by cancer types they are diagnosed with.
Differences in preference for forest healing programs according to gender
Difference of interest in forest healing depending on cancer types
There was a difference of interest in forest healing depending on the name of cancer types. The subjects with colorectal/breast/lung/liver/other types of cancer visited the forest once a week, those with thyroid/ovarian cancer once every 6 months, and those with gastric cancer once a year (Table 6). Those with breast cancer were most aware of forest healing programs, followed by other types of cancer, thyroid cancer, colorectal cancer, gastric cancer, lung/liver cancer, and ovarian cancer (Table 7). 45.1% (breast cancer, other types of cancer, lung cancer, colorectal/lung cancer, thyroid/gastric cancer, ovarian cancer) showed the intention to participate in the program, but 17.4% (breast cancer, gastric/lung/other types of cancer, lung cancer) did not (Table 8). For participation, 59.7% (breast cancer, other types of cancer, lung cancer, thyroid/colorectal cancer, gastric cancer, ovarian cancer, lung cancer) preferred mornings (49.3%) and afternoons (10.4%) on weekdays, 18.8% (breast cancer, thyroid/gastric cancer, colorectal/lung/other types of cancer, ovarian cancer) preferred Saturday mornings (15.3%) and afternoons (3.5%), and 7.7% (breast cancer, thyroid cancer, lung/other types of cancer) preferred Sunday mornings (5.6%) and afternoons (2.1%) (Table 9). The subjects with breast cancer, other types of cancer, thyroid cancer, colorectal/gastric cancer, ovarian cancer, and lung/liver cancer wanted to participate in the morning (Table 10). According to previous studies, it is necessary to develop programs that can increase the duration and desire to produce effects through forest activities depending on the characteristics of the subjects (Kim et al., 2015b), develop regular programs considering the characteristics of the subjects within 1–2 hours rather than non-regular programs depending on subjects, patterns, and operating method (Son et al., 2012), and subdivide the subjects according to the diagnosis by training experts in the relevant fields (forest health, forest exercise, forest experience in medicine, healthcare, nursing) (Hong and Lee, 2018). In this study, cancer patients showed a strong intention to participate in forest healing programs, and they tended to prefer mornings on weekdays. In further research, it is necessary to reclassify the patients by type of cancer and analyze their interest, preference, and needs to develop and implement scientific, systematic, sustainable, and regular forest healing programs based on the interest and healing factors, thereby ultimately improving the quality of the forest healing programs for cancer patients.
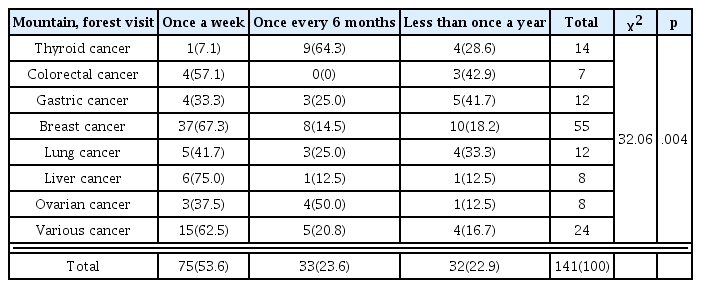
Differences in frequency of visits to mountains or forests according to cancer types

Differences in the perception of forest healing according to cancer types
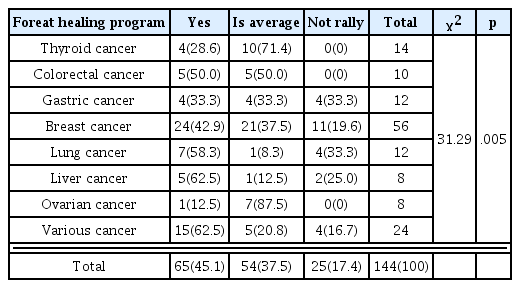
Differences in participating in forest healing according to cancer types

Differences in the desired day of the week to participate in forest healing according to cancer types
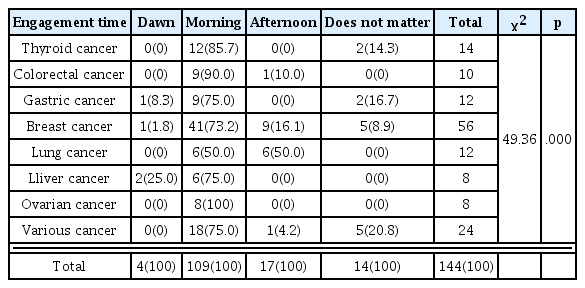
Differences in the desired time for participating in forest healing according to cancer types
Preference in forest healing program
The forest healing program most preferred by cancer patients was kinesiology (M = 4.39), followed by climate/water therapy (M = 4.11), diet therapy (M = 3.78), psychotherapy (M = 3. 76), and plant therapy (M = 3.45). The most preferred activity in kinesiology was walking through the forest (M = 4.47), forest exercises (M = 4.35), and laughter exercises (M = 4.22). In climate therapy, it was forest bathing (M = 4. 38), followed by natural meditation (M = 4.26) and wind bathing (M = 4.22). In water therapy, the most preferred activity was anion bathing (M = 4.02) and water sound listening and meditation (M = 3.85). In diet therapy, the subjects most preferred drinking tea (M = 4.32) and cooking with plants. In psychotherapy, the most preferred activity was abdominal breathing (M = 4.23), followed by lymphatic massage (M = 4. 13), and body scan (M = 3. 75) (Table 11). Activities in forest healing are classified by movement (static-dynamic), place (indoors-outdoors), five senses, therapy (plant, kinesiology, climate, psychotherapy, diet, water), and subject (general, chronic, environmental, toxic), but to actually apply them, it is necessary to develop programs depending on the diagnosis (Kim et al., 2019). Healing factors are classified into physical (water, sunlight, topography), chemical (phytoncide, anionic oxygen), sensory (sound, fragrance, taste, touch), and sociopsychological factors, and physical, physiological, sensory, and mental communion through forest healing factors promote physical and mental health (Kim et al., 2008). Activities that men and women most preferred in urban forests were forest bathing, wind bathing, and sunbathing, as well as looking at the natural landscape (Park and Koo, 2018). In this study, by developing and implementing a forest healing program that is suitable for the disease and characteristics of cancer patients using forest healing factors of kinesiology, climate therapy, water therapy, psychotherapy, and plant therapy preferred by cancer patients, it would be possible to provide effective programs for cancer patients with a high level of satisfaction.
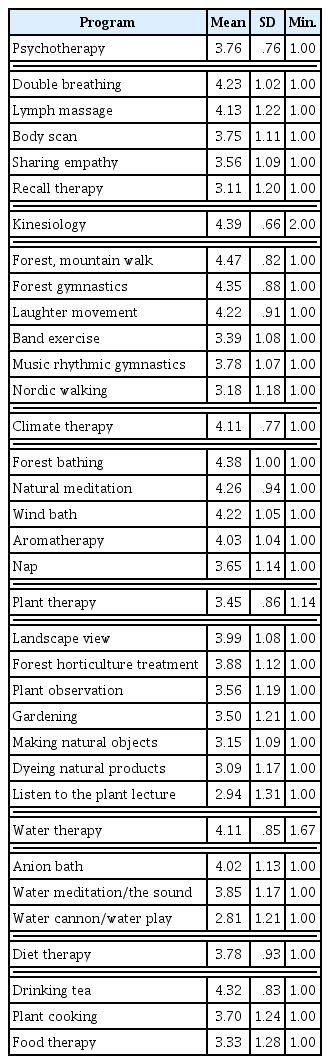
Forest healing program preference
Difference of preference in forest healing depending on gender and cancer types
As a result of conducting an independent samples t-test to verify the difference of preference in forest healing program by gender, it was found that there was a significant difference in diet therapy by gender (t = −2.96, p < .01). Women more preferred diet therapy than men, whereas there was no significant difference in psychotherapy, kinesiology, climate therapy, plant therapy, and water therapy (Table 12). There was also no significant difference of preference in forest healing program by cancer types. The healthy group of subjects preferred a sensitive approach using five senses depending on their stress level, whereas the risk group required help from specialists with a cognitive (lecture, counseling, coaching) approach (Kim, 2016a). In urban forests, participants preferred forest bathing, wind bathing, meditating, listening to the water, and foot bathing. Their biggest purpose of participation was to refresh themselves, relax, and promote health. Most men and women most preferred forest healing factors and attached great importance to forest healing programs and instructors (Park and Koo, 2018). In this study, female respondents preferred diet therapy. In further research, it is necessary to accurately determine the preferences of male and female cancer patients and scientifically develop and implement forest healing programs for each therapy based on advice from specialists (forest health, forest exercise, forest experience in medicine, healthcare, nursing), depending on the characteristics of the subjects.
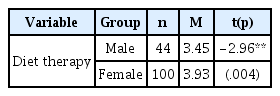
Differnces in preference for forest healing programs according to gender
Preference in the purpose of forest healing programs
For the purpose of participating in forest healing programs, the subjects most preferred the psychological (M = 4.26) domain, followed by physical (M = 3.76), social (M = 3.68), and cognitive (M = 3.64) domains. They had high expectations for relieving anxiety and depression through forest healing programs in the psychological aspect, relieving pain in the physical aspect, improving leisure in the social aspect, and improving concentration and sensory perception ability in the cognitive aspect, but there was no significant difference of preference in the purpose of forest healing programs by gender and cancer types (Table 13). To promote mental healing through social, psychological, and physical adaptability using plants, it is necessary to subdivide the aspects into emotional, social, cognitive, and physical domains depending on the subjects, purpose, and place, which are promoted by interactions (Relf, 1998). Depending on the stress level, the healthy group preferred walking in the forest, listening to the water, and experiencing the five senses, whereas the high-risk stress group preferred cognitive programs such as lectures, counseling, and coaching (Kim, 2016a). Among factors that affect psychosocial adaptation of cancer patients, stress has a direct effect; thus, not only the process of curing cancer but also psychosocial adaptation to coping with the process is important (Oh and Jang, 2014). To increase the therapeutic effects for cancer patients, it is necessary to first develop forest healing programs that meet the purpose of the treatment by reflecting the specificity of cancer types. Cancer patients need forest healing programs that can promote both their psychological stability and physical health, which requires systematic and scientific verification and analysis on the cancer types that the subjects are diagnosed with as well as the symptoms.

Preference for forest healing programs
Conclusion
This study was conducted to develop and implement differentiated forest healing programs by analyzing the preferences and needs of cancer patients and increase the effects of the programs. Thus, we conducted a self-administered survey from October 2018 to April 2019 on the subjects diagnosed with cancer. The sample size (n = 144) was the appropriate size required by G-Power, and the retrieved responses were analyzed using SPSS 25.0. 87% (120 subjects) were aware of forest healing programs, most of them from TV, followed by the internet and SNS. 79.2% (114 subjects) did not have experience participating in a forest healing program, but 82.6% (118 subjects) had intention to participate. This indicates that even though not many of them have experience participating in forest healing, they showed high interest and needs for participation. They preferred to participate in spring (29.9%) and fall (27.8%), in programs carried out for 1.5–2 hours in the morning on weekdays, which suggests the need to develop various programs using forests in the four seasons. In the needs for forest healing programs, the subjects most preferred kinesiology, followed by climate therapy and water therapy, then diet therapy, psychotherapy, and plant therapy. Exercise programs for cancer patients will help lower their depression and increase resilience through engagement in nature as well as various physical and emotional activities. Moreover, subjective, direct activities in the physical environment of a forest will have positive effects on improving the physiological functions and lifting the mood. For the purpose of participation, the subjects most preferred the psychological domain, followed by physical, social, and cognitive domains. This indicates that, although this study is limited as it is conducted on 144 cancer patients without enough male respondents, surveying the needs and purposes of cancer patients is significant in that it has raised the need for continuous research on development and implementation of forest healing programs. Furthermore, developing manuals from implementation of forest healing programs is an inevitable task to improve the effects of forest healing. This study failed to classify many cancer types for statistics as it was difficult to obtain a greater sample size due to the nature of the subjects, and thus it is necessary to conduct a more systematic survey by classifying the diagnosis. Further research must provide ways to plan, develop, and implement differentiated forest healing programs considering the psychological and physical characteristics of cancer patients as well as the natural environment. It is first necessary to develop forest healing programs that meet the therapeutic purposes based on surveys on the needs and purposes of the programs according to the classification of diagnosis for the five main types of cancer (gastric cancer, colorectal cancer, liver cancer, breast cancer, cervical cancer) in the national cancer policy. There is also a need to plan forest healing program that can promote both psychological stability and physical health of cancer patients and verify and evaluate their effects based on specialized training of forest healing instructors.