Effects of Forest Healing Program on Depression, Stress and Cortisol Changes of Cancer Patients
Article information
Abstract
Patients diagnosed with cancer face mental problems such as alienation, isolation, anxiety about death and fear, recovering from psychological difficulties. In this study, a forest healing program was provided for cancer patients to recover from psychological stress, depression, social isolation and self-esteem caused by cancer and changes in salivary cortisol through psychological and emotional recovery were measured.
From September 19 to November 28, 2017, a forest healing program composed of a total of 10 sessions, two hours per session was provided for 12 cancer patients in the Forest of Taegyo located in Yongin. Psychological tests were performed with Social Adaptation Self-evaluation Scale (SASS), Korean-version Perceived Stress Scale (PSS) and Beck Depression Inventory (BDI) and the collected data were analyzed with the SPSS 18.0. The salivary cortisol level was measured along with the psychological tests and were analyzed by a specialized testing agency. The results of the analysis showed that the pre- and post-assessment score of SASS was 29.17 and 25.92, respectively, and that the pre- and post-assessment score of PSS was 30.50 and 23.92, respectively. The pre- and post-assessment score of BDI was 41.00 and 34.83, respectively, which showed significant differences. In addition, the pre- and post-assessment level of saliva cortisol was 3.13 and 1.68, respectively, showing a significant decrease. In short, the forest healing program was found to be effective in reducing physiological changes caused by social isolation and stress due to the emotional and psychological difficulties that the subjects who were diagnosed with cancer and were recovering from it have. In the future, it will be necessary to develop and implement a forest healing program by conducting a forest healing requirement survey on cancer patients.
Introduction
Despite the development of medical skills in modern society, the number of cancer patients has been on the rise. The number between 1999 and 2017 was 1,867,405, and 819,837 were males (43.9%), and 1,047,567, females (56.1%). Gastric cancer topped the list of male cancer patients, followed by lung cancer, colorectal cancer, prostate cancer and liver cancer, while breast cancer topped the list of female cancer patients, followed by thyroid cancer, colorectal cancer, gastric cancer and lung cancer (National Cancer Information Center, 2018). Regardless of gender and age, cancers can be developed in any part of the body, and most of the patients who are diagnosed with and fight against cancers experience a variety of emotional changes such as anxiety, fear, depression, psychological stress and despair due to anxiety and fear over physical distress, death and parting with family members, which lowers their self-efficacy (Anderson, 1989; Koh and Kim, 1988; Lee, 2017; Yu, 2016). After being diagnosed with cancers, cancer patients receive chemotherapy, surgery or radiotherapy, and in the process psychological, physiological and physical changes and pain are accompanied, and acute and chronic stress caused by the changes affects the secretion of cortisol, a type of hormone (Hockenberry-Eaton et al., 1994).
Depression accompanied with cancers has a negative impact on cancer survival and treatment performance, and utilizing forests and natural objects as an intervention method for treating and recovering health from diseases and reducing symptoms was reported to have a positive impact on self-realization and to be effective in relieving depression (Shin, 2007). As various activities in forests reduce stress and increase alpha waves, they can be utilized as a means of physiological and psychological therapy and affect immune functions (Park, 2010). Active activities using forests induce positive emotions, improve emotional stability and physical resilience, and thus are effective in reducing stress (Jeon and Shin, 2017). Forest healing programs that improve the health of the body and mind and reduce depression using natural objects and phytoncides released from forests lower the level of cortisol, a stress hormone, induce deep sleep and activate the functions of NK cells, which is effective in boosting immunity (Kim et al., 2011).
Forest therapy involves all the activities that improve the health of the body and mind utilizing therapeutic elements that forests have, and of which effects were scientifically proven (Park, 2010). They include physical activities such as hiking, walking, stretching exercises, yoga and meditation, and medicinal elements such as edible and medicinal plants and wild plants (Korea Forest Service, 2011). Forest healing elements such as forest landscape, phytoncides, anions, oxygen, sound, sunlight, etc. are natural elements that forests have and they are involved in forest activities that improve the health of the body and mind. Forest therapies can be divided into 6 groups: phytotherapy; hydrotherapy; climatotherapy; dietary therapy; kinesi-therapy; and psychotherapy (Kim, 2006). Walking like hiking was reported to improve breast cancer patients’ quality of life by improving physical, psychological and social functions through physical intervention, and lack of physical activities is recognized as a risk factor of cancer (Chae et al., 2002). Activities in urban forests are associated with cancer patients’ dynamic of physical activities, and are an important condition for their independence through physical and psychological recovery (Kim, 2014). This study provided a forest healing program that utilized forest healing elements for cancer patients who were experiencing mental and physiological stress in the process of receiving therapies and treatments such as surgery and medicinal therapy after being diagnosed with cancer, and examined psychological and social stress and depression and changes in the level of cortisol.
Research Methods
Subjects
The forest healing program was provided for a total of 16 subjects (eight males, eight females) who participated in a self-help organization for cancer patients in Yongin-si, Korea. They were informed of the purpose of this study and the forest healing program, and they voluntarily signed a consent form prior to participating in the program. In the middle of the program, four subjects (one male, three females) dropped out of the program, and a total of 12 subjects (seven males, five females) completed the program. The general characteristics of subjects who participated in the forest healing program were as shown in Table 1.
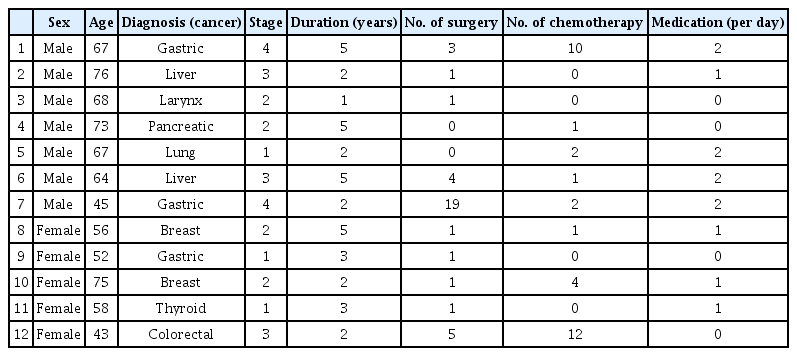
General characteristics of the study subjects
Duration and program
The forest healing program was operated from September 19 to November 28, 2017 in the Forest of Taegyo located in Yongin where Larix kaempferi, Chamaecyparis obtusa, Quercus trees, Acer palmatum and Pinus densiflora are distributed, and a total of 10 sessions were provided, 2 hours per session. Forest healing elements including forest landscape, phytoncides, anions, oxygen, sound, sunlight, etc. and six therapy types were applied to healing activities (Kim, 2006), and the detailed program content was designed based on earlier studies (Table 2). That is, walking on forest trails, strolling, landscape viewing, and games using natural objects were included, and two Grade-1 forest therapists and one nurse attended each session. A total of 10 sessions, 2 hours per session, were provided (Table 3). The Grade-1 forest therapists led the program and instructed participants to bring rainbow-colored clothes and objects to increase their participation in each session.
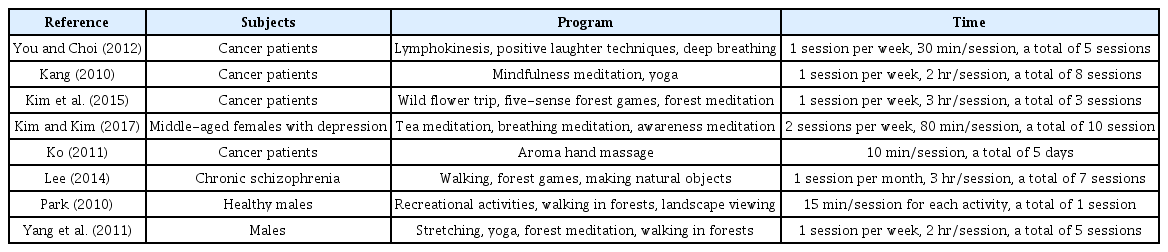
Analysis of the preceding thesis program
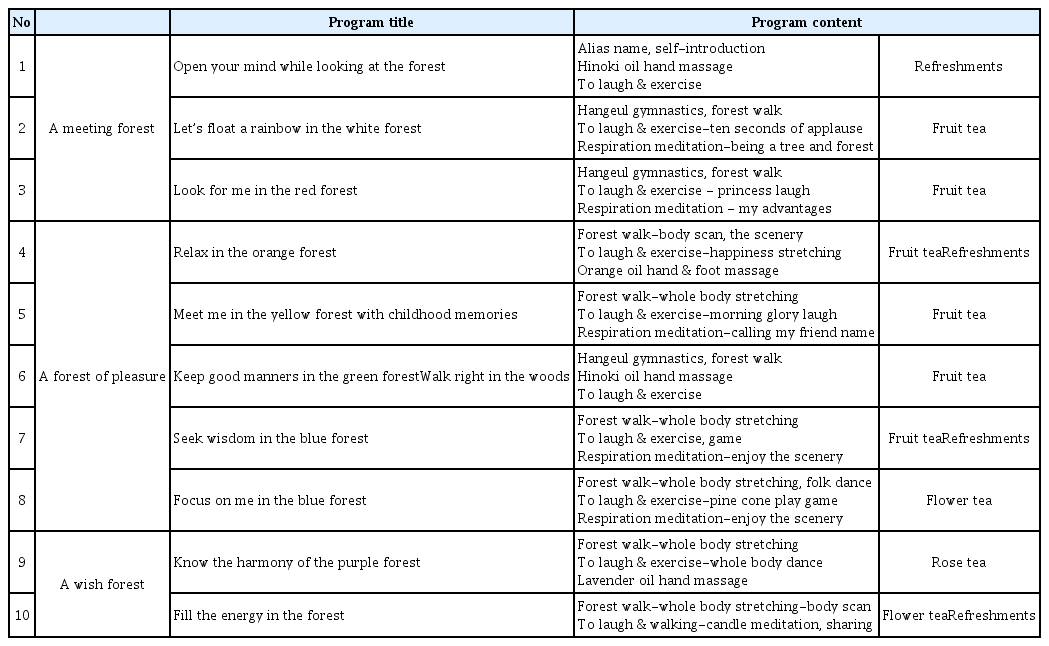
Forest healing program by session
Assessment tools
Beck Depression Inventory (BDI)
Beck Depression Inventory (BDI) is a test to distinguish depression from anxiety (Beck and Beck, 1972), and is a self-rating scale composed of a total of 21 questions developed to measure overall depressive symptoms including psychological, cognitive, motivational and physiological symptoms. Several sentences on the level of depressive symptoms were presented to subjects, and they chose those that described the best their experience for the past one week. The results are interpreted as the higher the score, the higher the level of depression. Depending on the type and level of depression, subjects score their symptoms as follows: never or hardly ever, 1 point; sometimes, 2 points; often, 3 points; and almost constantly, 4 points. The score ranged between 0 and 9 means no or minimal depression; 10–15 points, mild depression; 16–23 points, moderate depression; and 24–63 points, severe depression. The higher the score, the higher the level of depression. The inter-item consistency coefficient was .87.
Perceived Stress Scale (PSS)
Perceived Stress Scale (PSS) was developed to measure the subjective level of stress (Beck et al., 1961), and in this study the Korean standardized version was used (Park and Seo, 2010). PSS was composed of five negative questions and five positive questions including those about whether to feel uncontrollable and excessive pressure and the level of stress that subjects feel currently, direct questions on the level of stress, focusing on general situations rather than a certain event. A Likert 5-point scale (from ‘hardly ever; 1 point’ to ‘very frequently; 5 points’) was used, and a total score was calculated. The higher the score, the higher the level of self-perceived stress. The inter-item consistency coefficient was .84 for positive perception, .81 for negative perception, and .88 for self-perceived stress.
Social Adaptation Self-evaluation Scale (SASS)
Social Adaptation Self-evaluation Scale (SASS) is designed to assess the social adaptation of depression, and is composed of 21 questions (Bosc et al., 1997) on the following items: activeness and confidence in social activities and occupation; importance of appearance; joy and interest; relationship within family and external relationship; intellectual interest; role satisfaction; and abilities related to resources and finance. Using the scale, social activities self-perception and intellectual exploration, and satisfaction with and interest in role can be assessed. Each question is scored as follows: very high (3 points); moderate (2 points); little (1 point); and ‘none (0 point),’ and a total score is calculated. This scale is a useful tool for assessing the social adaptation and activeness of patients with depression. The lower the score, the more positive social adaptation. The inter-item consistency coefficient was .75 for social activities, .78 for self-perception, .78 for interest in role, and .84 for self-rated social adaptation.
Cortisol
Cortisol is an adrenocorticotropic hormone (ACTH). When people face an external situation like stress, the hypothalamus in the diencephalon detects it first, and corticotropin-releasing hormone (CRH) is secreted and stimulates the pituitary gland. The pituitary gland in turn secretes an adrenocortisoltropic hormone, called cortisol. Measuring cortisol is an objective way to assess mental and physical stress. Salivary cortisol analysis is a good tool for studies on stress and diseases focusing on the activity of the sympathetic nervous system and the hypothalamic-pituitary-adrenal axis (Ahn et al., 2007). In particular, blood collecting can induce stress in those who were diagnosed with cancer and had experience of treatment and surgery in hospitals, and salivary cortisol, unlike that associated with albumin, is in the form of free molecules. The biochemical analysis method can minimize the additional generation of stress (Yun, 2007).
Data collection and analysis methods
The forest healing program was operated from September 19 to November 28, 2017, a total of 10 sessions, 2 hours per session. Pre-assessment was performed before starting the 1st session, and post-assessment was performed after completing the 10th session. BDI, PSS and SASS for subjects’ psychological assessment were performed respectively after collecting cortisol data in order not to affect the collection of cortisol. The surveys were performed using a self-administrated questionnaire survey method, the pre-assessment was performed at 9:45 AM before starting the 1st session on September 19, and the post-assessment was performed at 12:30 PM after completing the 10th session on November 28. Salivary cortisol, a stress hormone, was collected for pre-assessment at 9:30 AM, 30 minutes before starting the 1st session on September 19, and for post-assessment 10 minutes after completing the last session at 10 PM on November 28. For 1 hour prior to collecting salivary cortisol, any food intake was prohibited, and subjects were instructed to rinse their mouth with water before collecting saliva. The parotid gland was stimulated through massage and the sublingual gland was stimulated through tongue movement to ensure a sufficient amount of saliva is produced. Salivary samples were collected using the Salivary Cortisol ELISA Kit (Salimetrics, USA). Subjects placed a sterilized cotton pad in the mouth, and after the cotton pad absorbed saliva sufficiently (about 2 ml), the cotton pad was placed and sealed in a container, was transferred to the laboratory of Korea Air Force Academy under refrigeration, and was analyzed within 24 hours.
All the collected data were statistically analyzed using the SPSS 18.0 program, and the inter-item consistency coefficient was calculated to test the reliability of the self-administered questionnaire survey. Descriptive statistical analysis was performed on the general characteristics of subjects, and the data collected from the pre- and post-assessment of BDI, PSS, SASS, and the data of salivary cortisol analysis were analyzed using the Wilcoxon Signed-Rank test.
Results and Discussion
Changes in Beck Depression Inventory (BDI)
The effects of the forest healing program on changes in the depression of cancer patients were analyzed as shown in Table 4. The BDI before and after operating the forest healing program was 41.00 and 34.83, respectively, which shows a significant difference and can be interpreted that depression was reduced. This can be attributed to the positive effects of walking using forest features and hands-on experience games utilizing forest resources on refreshing feelings, and interactive activities with others such as laughter exercises and hand massage also seemed to have a positive impact on subjects’ psychological and physical conditions. An earlier study on the effects of forest-experience-integration programs on the depression and resilience of community dwelling cancer patients (Choi and Ha, 2014) also reported that physical exercise intervention through walking on forest trails reduced depression of cancer patients, improved their resilience and thus improved their quality of life, which coincided with the results of this study.

Comparisons of cancer patients’BDI before and after forest healing program
Changes in Perceived Stress Scale (PSS)
The effects of the forest healing program on changes in the perceived stress of cancer patients were analyzed as shown in Table 5. The PSS before and after operating the forest healing program was 30.50 and 23.92, respectively, which shows a significant decrease. As a sub-item, pre- and post-positive perception was 15.75 and 11.333 respectively, showing a positive decrease, and pre- and post-negative perception was 13.17 and 11.58, respectively, showing a significant decrease. Negative stress is the level of stress that individuals feel unpredictable, uncontrollable, and overpowered in daily life, and positive stress is the level of stress that individuals feel they can predict, control and successfully handle things that occur in daily life (Park and Seo, 2010).
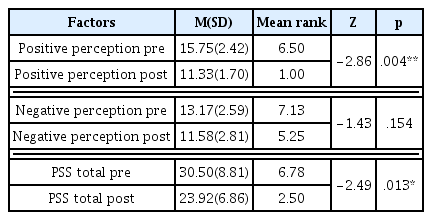
Comparisons of cancer patients’PSS before and after forest healing program
Forest activities have a positive impact on the independence of cancer patients through physical and psychological recovery, reduce stress and refresh the mind and body (Kim, 2014), and forest healing programs refresh the feelings of cancer patients and relax their mind and body, reducing stress (Son, 2019). In addition, laughter therapies for cancer patients relieve anxiety and stress and reduce depression (Kim, 2019). Mindfulness was also reported to reduce cancer patients’ stress perception and improve self-management abilities (Kang, 2010).
Changes in Social Adaptation Self-evaluation Scale (SASS)
The effects of the forest healing program on changes in the stress of cancer patients measured through the SASS were analyzed as shown in Table 6. The pre- and post-SASS was 29.17 and 25.92, respectively, showing a positive improvement. As a sub-item of SASS, pre- and post-self-perception was 9.42 and 9.00, showing no significant change after operating the forest healing program. However, pre- and post-activity was 11.00 and 9.67, respectively, and pre- and post-role interest was 11.08 and 9.50, respectively, which indicates that subjects’ self-assessment on social activities and role interest was improved. Since cancer patients’ psychological problems are interrelated with physical problems and cause depression, people tend to think that cancer patients might suspend their occupation or hobby in the process of being diagnosed with cancer and receiving treatment and might be passive toward social functions and activities. Unlike the prejudice, these positive changes show that they enjoy hobbies and leisure activities through which they receive others’ help, have a sense of satisfaction through social contact and enjoy their life, which can be attributed to positive changes in social activities after participating in the forest healing program.

Comparisons of cancer patients’SASS before and after forest healing program
Changes in Cortisol
The effects of the forest healing program on cancer patients’ stress hormone were analyzed as shown in Table 7. The level of cortisol before and after operating the forest healing program was 3.13 and 1.68, respectively, showing a great decrease. Cortisol is an adrenal hormone that is secreted from the adrenal of the kidney under stress. The primitiveness of forests has a positive effect on the autonomic nervous system and the endocrine system, and physical activities in green spaces are known to be effective in reducing stress (Choi and Ahn, 2015). A one-day forest healing program provided for patients with chronic schizophrenia was found to reduce the level of cortisol more in October than April and July (Lee, 2014), and even only walking for 15 minutes in forests reduced the level of salivary cortisol (Park, 2010). A forest healing program provided for females after menopause was found to be effective on the salivary cortisol concentration until 2 weeks after finishing the program, and the salivary cortisol concentration started to gradually change after 4 weeks (Yu, 2016).
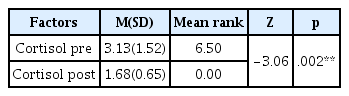
Comparisons of cancer patients’cortisol before and after forest healing program
Conclusion
This study planned a forest healing program that utilized forest therapeutic elements for cancer patients in Yongin-si, Korea who suffer from physiological and mental stress in the process of receiving treatment after being diagnosed with cancer. A total of 10 sessions were operated once a week from September 19, 2017 in the Forest of Taegyo located in Yongin to examine psychological and social stress and changes in cortisol, a physiological hormone.
After operating the forest healing program, the results of BDI showed statistically significant differences, which can be attributed to the positive effects of walking and activities that utilize natural objects in forests on physical and psychological changes caused by cancer surgeries. The results of PSS also showed a significant decrease, and changes in positive perception, a sub-item of PSS, showed a significant decrease, which can be attributed to the improved abilities of predicting, controlling and handling events in daily life. The PSS questionnaire was conducted to predict and prevent serious psychological problems such as depression, anxiety and suicide, and the stress that subjects experienced within one month. It is difficult to accurately measure stress caused by pain that cancer patients experience, but reducing depression and anxiety seemed to have a direct impact on the improved quality of life. The results of SASS showed a statistically significant decrease, and social activities, self-perception and role interest as sub-items were significantly improved. Natural activities seemed to enable cancer patients sympathize with other cancer patients and immerse themselves both physically and mentally, contributing to their social adaptation. Cortisol, a physiological hormone secreted under stress, was significantly reduced, and the forest healing program seemed to be very positive for changes in cancer patients’ cortisol level.
As the results above indicate, the mental problems of cancer patients combined with their physical problems cause depression, and for this reason forest healing programs that can relax their mind and improve their physical motor abilities have positive effects on them through active activities that can arouse their interest utilizing forest resources. It was difficult to conduct functional assessment on social activities due to the characteristics of cancer patients in this study, but it is necessary to develop a questionnaire for assessing social interest and functions. Unlike the prejudice that patients might be passive, subjects showed interest in sociality and role interest, and it is necessary to develop forest healing programs that enable them to enjoy their life with satisfaction and confidence by providing opportunity for contacting with society through hobbies and leisure activities.
It will be necessary to survey and analyze cancer patients’ interest in and demand for forest healing considering their characteristics, and to plan and develop specialized programs for cancer patients based on the results of the analysis. In addition, those programs need to be led by forest therapists with professional knowledge, and the inflammation index of cancer patients also needs to be measured through a blood test during their physiological test. Since this study was conducted on a limited number of samples, a careful approach is required to generalize and explain the effects of forest healing programs for all the cancer patients in Korea, but the results are expected to be the foundation for the activation, research and development of forest healing programs.