Research Trends on the Effects of Forest Therapy in Korea and Ways to Improve the Level of Medical Evidence: A Scoping Review
Article information

Abstract
Background and objective
Studies on the effects of forest therapy are clinical research that reveals the effects suitable for the purpose of therapy by applying a forest therapy program, which is a complex intervention, to humans in various forest environments. Accordingly, the purpose of this study is to find out the characteristics of existing studies on the effects of forest therapy and to suggest ways to improve the level of evidence for future research results. In this study, a scoping review was conducted to find out how studies on the effects of forest therapy were conducted based on the medical clinical research method in domestic studies on the effects of forest therapy.
Methods
The scoping review utilized a procedure proposed by the Joanna Briggs Institute (JBI). A total of 564 studies were searched and 57 were used in the final analysis.
Results
As a result of the analysis, only 1 study (1.8%) had a manual to reproduce the forest therapy program, and 56 studies (98.2%) reported only brief information on the program. As for the report on forest therapy environments, there were articles that mentioned some therapy environments, but none predicted the effects or reported about reproducibility. Among the reports on forest therapy environments, 21.1% reported about both forest and thermal environments, and 26.3% reported only about the forest environment.
Conclusion
From the perspective of clinical research, the level of evidence for studies on the effects of forest therapy so far has been found to be very low, and methods for applying clinical research methods to improve this have been discussed. Clinical research is a prerequisite for verifying medical effects in order to raise the level of forest therapy from wellness to treatment support activities, and it must be actively utilized in the future.
Introduction
Human lifespan is increasing with the advancements in modern science and health technology. Accordingly, the paradigm for life has shifted from living long to living healthy (Korea Tourism Organization, 2018). The scope of medical care has also expanded from focusing on treatment at medical institutions to improving the quality of life by increasing the level of health (Lee et al., 2014). More and more people are enthusiastic about managing their health through healing and leisure, and each country is establishing and implementing health and medical care policies with the goal of increasing the levels of national health and improving the quality of life (Jung, 2012). With this social trend, there has been a continuous increase of research that verifies the physiological, psychological, and social impacts of the natural environment and nature-based activities on the human body (Yoo et al., 2015; Global Wellness Institute, 2022). With the cumulative research findings on the fact that nature-based programs have a positive impact on the human body, nature-based activities have been receiving attention also in terms of preventive medicine (Li and Kawada, 2014; Song et al., 2016).
With the growing awareness of the value and importance of natural medicine using forests in South Korea, the Forestry Culture and Recreation Act was amended in 2012 so that it includes the concept of forest therapy and contents about training forest therapy experts. The forest therapy industry with established legal grounds later increased the formation of Healing Forests and has come to develop and run various forest therapy programs using forest therapy experts (Park et al., 2021a). As a result, more and more people could experience Healing Forests and forest therapy programs, and analytical studies on them have also been conducted. These studies analyzed that people have a positive perception towards the health benefits of forest therapy, and that activities in forests have the effect of reducing the annual number of hospital visits as well as medical expenses. For this reason, it is suggested that forest therapy has the potential to be used in medical environments (Park et al., 2014; Lee et al., 2015).
In addition, studies on forest therapy are conducted by analyzing its effect on health promotion through diverse subjects (Song and Bang, 2017; Lee et al., 2023; Lee et al., 2016; Chae and Lee, 2020), and continuous efforts are made to reveal the acceptable medical effects in health and medical care (Park et al., 2021b). However, there has been no explicit agreement on the concept of the medical effects of forest therapy or the research methods to reveal them. There is also no analysis about whether studies on the effects of forest therapy have reasonable evidence for revealing the medical effects. According to existing systematic reviews that analyze the medical effects of forest therapy through research synthesis, there are case studies on forest therapy showing physically, mentally, and socially positive effects. However, there is insufficient research applying rigorous experimental designs, and many studies merely compared before and after intervention without a control group, making it difficult to prove the medical effects. Moreover, it is also not easy to evaluate the effect size due to the large heterogeneity between interventions (Lee et al., 2017; Chae and Lee, 2020; Stier-Jarmer et al., 2021).
Research on forest therapy is focused on establishing a scientific basis by discovering objective and quantitative indicators (Song et al., 2016). Studies on humans have various matters to consider along with the ethical aspect from the research planning stage in addition to the scientific research methods. Moreover, since bias is highly likely to interfere with the research process, there is a need for rigorous research design and implementation process to obtain valid conclusions (Park, 2005; Chang et al., 2013).
Research investigating the effects of forest therapy prospectively identifies physically, psychologically, and physiologically positive changes by developing and applying forest-based therapy programs for people, which meets the requirements for clinical research set by the National Institutes of Health (NIH). In other words, studies on the effects of forest therapy are definite clinical research, and thus it is necessary to apply not only scientific research methods but also medical clinical research methods to analyze the effects of forest therapy programs on the human body. Applying these research methods not only reveals the medical effects of forest therapy but also provides clear academic evidence. There is a need to identify the key concepts, methods, and characteristics used in research by analyzing studies on the effects of forest therapy conducted thus far in order to apply medical clinical research methods.
Accordingly, this study conducted a scoping review to examine the characteristics and contents of studies on the effects of forest therapy conducted in South Korea from 2012, when the Forestry Culture and Recreation Act was amended, to May 2023. In this study, we intend to find out how studies on the effects of forest therapy are conducted by identifying the concepts of effects used in such studies, as well as the research methods and the characteristics and contents of forest therapy programs based on medical clinical research design methods. Through this process, we will present the concepts of medical effects of forest therapy and provide evidence and plans of clinical research methods for forest therapy to investigate its medical effects. This is to propose the direction and framework for theoretical discussion of clinical research methodologies to improve medical evidence in forest therapy.
Research Methods
Research design
This study is a scoping review that analyzes the key concepts used in domestic studies on the effects of forest therapy and identifies the current status and characteristics of research methods and forest therapy programs. A scoping review one of the research methods that integrate evidence to address specific research questions after strictly and systematically searching available literature (Peters et al., 2020). In particular, it is suitable for the purpose of clearly identifying key concepts and definitions and determining how research on specific topics or fields is being conducted (Munn et al., 2018), and it is a method that can present clear and specific contents for further research based on the findings obtained as a result of the review (Peters et al., 2015). This study was conducted according to the scoping review procedures provided by the Joanna Briggs Institute (JBI), and the report of the literature search results was conducted according to PRISMA-ScR (Preferred Reporting Items for Systematic reviews and Meta-Analyses extension for Scoping Reviews), which is an extended set of report guidelines for scoping reviews (Tricco et al., 2018).
Research questions and selection criteria
The research question in this study is: "How are the concepts of effects, characteristics of forest therapy research design methods, major characteristics of interventions in forest therapy programs, and characteristics of the environment in which forest therapy programs are provided reported in domestic studies on the effects of forest therapy?" The specific questions are as follows.
First, how is the concept of effect used in domestic studies on the effects of forest therapy?
Second, what research methods are used in studies on the effects of forest therapy to measure and analyze the effects?
Third, how are therapeutic interventions to prove the effects, i.e., forest therapy programs, defined and reported in research?
Fourth, are there reports about the environment in which forest therapy programs are provided?
The selection criteria for data included in this scoping review are as follows: ➀ research conducted domestically and published in domestic and international journals, ➁ research that measured health-related effects on humans, ➂ research involving forest-based interventions, and ➃ research implementing forest therapy programs consisting of a combination of unit programs.
Literature search and selection
Literature search
Literature search was conducted on journal articles published in Korean and English in Korea and abroad from 2012 to May 2023. Domestic databases such as the Research Information Sharing Service (RISS), Korean Studies Information Service System (KISS), and DataBase Periodical Information Academic (DBpia) and international databases such as PubMed and ProQuest Medical Library (PML) were used to search published literature. The search terms for domestic journals were "effect of forest therapy" OR "impact of forest therapy", and the search terms for international journals were "forest therapy" OR "forest intervention" OR "forest activity" AND Korea [Affiliation]. Boolean operators AND/OR and truncation were applied for search depending on the characteristics of each database, and the search period was from June 1 to June 28, 2023.
Literature selection
This literature search and selection process was conducted according to the guidelines presented in the PRISMA 2020 statement (Page et al., 2021). Total 564 articles were reviewed by searching domestic and international databases: 201 articles on RISS, 125 articles on KISS, 141 articles on DBpia, 46 articles on PubMed, and 51 articles on PML (Fig. 1). The duplicate search function of bibliographic management program EndNote 2.0 was used to primarily exclude 256 duplicates, after which we secondarily excluded 42 duplicates. After excluding 191 articles that do not meet the selection criteria, we excluded 19 articles for which the full text cannot be retrieved, and 5 articles that belong to the exclusion criteria, thereby selecting 51 articles. We then additionally identified 6 articles through the process of reviewing the list of references for the articles studied, and applied the same review process as above to the 6 articles and added them to the final list. Total 57 articles were ultimately selected through the literature search process above.
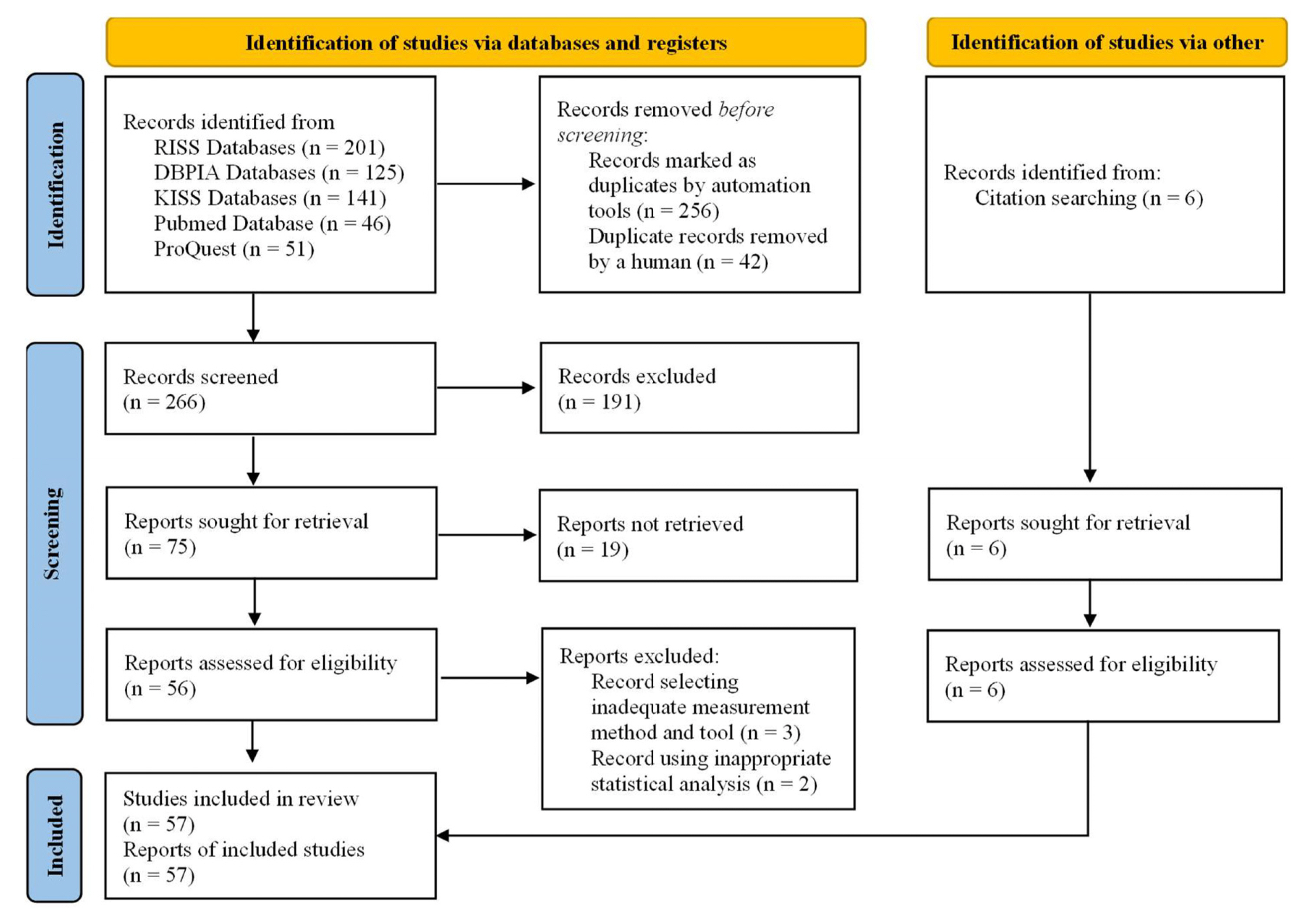
Flowchart of study selection process.
(Source: http://www.prisma-statement.org/PRISMAStatement/FlowDiagram)
The exclusion criteria were: ➀ articles for which the full text cannot be retrieved such as conference proceedings and ➁ articles for which two experts simultaneously suggested exclusion, to which a third expert agreed. The articles excluded were 3 articles selecting inadequate measurement methods and tools, and 2 articles using inappropriate statistical analysis.
Literature review process
We coordinated 20 articles to increase consistency between researchers prior to the literature selection process. Two researchers reviewed the same 20 articles, discussed the results, and developed and revised the data extraction manual for analysis. Then, the two researchers independently reviewed the titles, abstracts, and full texts in order and applied the selection criteria. When the two researchers made different judgments about study selection and data extraction, the relevant articles were reexamined and discussed to make the final decision.
Data extraction and analysis
Two researchers independently extracted and confirmed data from the selected articles according to the data analysis framework developed in advance using a Microsoft Excel sheet. The data analysis applied to this study was divided into the general characteristics of the study, characteristics of the research method, characteristics of the intervention that is the forest therapy programs, and the characteristics of the environment in which forest therapy programs were provided.
The general characteristics of the study were organized by publication year, research subjects, and the concept of effect described in the research purpose.
Data were extracted based on the design of clinical research to investigate the medical effects (Park, 2005; Chang et al., 2012). Data were analyzed by classifying ethical considerations of the study, research method, sample size, and interventions applied to the control group in case the study had a control group. For ethical considerations, we checked whether the study passed the deliberation of the Institutional Review Board (IRB) presented in the study and whether the subjects agreed, and applied the IRB deliberation information as a superordinate concept when reporting duplicates. For the research methods, the analysis was conducted based on DAMI 2.0 (study Design Algorithm for Medical Literature of Intervention 2.0), a clinical research literature classification tool developed for systematic review by Health Insurance Review and Assessment Service (Health Insurance Review and Assessment Service, 2013). The research methods were classified into randomized controlled studies (RCTs), non-randomized controlled studies (non-RCTs), and before-after studies, which are defined as shown in Table 1.

Research design methods and definitions
The characteristics of the interventions were extracted based on the TIDieR (Template for Intervention Description and Replication) checklist, a reporting guideline for intervention studies presented by the EQUATOR Network (Enhancing the QUAlity and Transparency Of health Research), which provides tools related to health research in international medicine (Campbell et al., 2018). Data were derived by identifying whether the forest therapy program used in the study was organized based on theoretical grounds and mechanisms or previous studies, whether there is a manual or protocol for the provider to reproduce the forest therapy program equally and faithfully, whether there are the qualifications required for program operators, and what was reported about the explanations or information on the environment in which the program was provided.
Finally, data were extracted on the contents reported about the characteristics of the forest therapy environment. Reports about the forest environment and thermal environment were derived in detail among these characteristics for analysis.
Results and Discussion
General characteristics of studies
Total 57 articles were published and searched from 2012 to 2023: 39 from domestic journals, and 18 from international journals. By year of publication, there were 4 articles published in 2012 (7.0%), 3 in 2013 (5.3%), 4 in 2014 (7.0%), 5 in 2015 (8.8%), 1 in 2016 (1.8%), 4 in 2017 (7.0%), 3 in 2018 (5.3%), 4 in 2019 (7.0%), 7 in 2020 (12.3%), 9 in 2021 (15.8%), and 13 in 2022 (22.8%), showing that most were published in 2022. As for the journal index of selected studies, there were 36 articles from KCI-listed journals (63.2%), 15 from SCIE-listed journals (26.3%), 3 from Scopus-listed journals (5.3%), and 3 from KCI candidate journals (5.3%).
As for the subjects, 11 articles were on children and adolescents (19.3%), and 8 were on the elderly (14.0%). Most studies were targeting adults (33 articles, 57.9%), 5 of which were on college students, 1 on pregnant women, 9 on the middle-aged and older adults aged 40 to 70, and 18 on adults aged 18 to 65. There were 5 articles that recruited subjects who visited a forest therapy center regardless of age or diseases. As of 2023, the age standard for the elderly used by administrative agencies in South Korea is 65 and above, but the age standards for the elderly used in articles were broader, ranging from 60 to 70.
By research purpose, there were 15 articles (26.3%) in which forest therapy programs were implemented for the purpose of alleviating or improving symptoms caused by diseases. They included 3 articles on pain relief, 3 articles on alleviating depression due to diseases, 2 articles on improving sleep quality, 2 articles on alleviating depression, 2 articles on alleviating Internet addiction symptoms, and 1 article each on alleviating symptoms of hwabyeong (or hwa-byung), atopic dermatitis, and menopause (Table 2). In 42 articles excluding studies conducted to alleviate diseases or symptoms, the effects of forest therapy programs were evaluated by dividing them into psychological and physiological effects. There were 9 articles on specific occupational groups, conducted for the purpose of promoting mental health through psychological effects of forest therapy such as relief of stress and depression. Psychological effects were being evaluated with the concepts of stress reduction, positive and negative emotional changes, improved quality of life, improved self-esteem, reduced anxiety, reduced depression, emotional stability, and mental health recovery, while physiological effects were measured by heart rate variability (HRV), blood pressure, cortisol, and melatonin to determine physiological stability or NK-cell activity. There were also articles evaluating physical effects by analyzing body composition or measuring functional fitness, as well as articles evaluating cognitive effects through neurocognitive testing.

General characteristics of included studies (N = 57)
Characteristics of research methods
In the case of analysis for ethical considerations, 31 articles (54.4%) described that the research was approved by the IRB, 15 (26.3%) reported that they obtained consent from the research subjects, and 11 (19.3%) that did not report relevant information. As for articles published in international journals, all 18 articles reported that they were approved by the IRB. On the other hand, only 13 out of 39 articles published in domestic journals reported that they were reviewed by the IRB. There were 7 articles (12.3%) that selected samples by applying the sample size calculation method, 1 (1.8%) that selected the sample randomly, and 49 (86.0%) that did not report relevant information. Most articles were before-after studies (28 articles, 49.1%) comparing before and after forest therapy programs of a single group, followed by non-RCTs (18 articles, 31.6%) and RCTs (11 articles, 19.3%) (Table 3). Out of 29 comparative clinical studies applying a control group, 17 articles applied no treatment or daily life as comparative intervention of the control group, followed by 6 that provided different interventions in both programs and locations and compared them, 5 that applied the same program but only different locations and compared them, and 4 that applied different programs in the same location.

Research method characteristics of included studies (N = 57)
Characteristics of forest therapy programs
There were 48 articles (84.2%) that reported the purpose of the forest therapy programs, which are interventions used in the study, and 9 (15.8%) that did not report relevant information. 20 articles (35.0%) reported that they applied theories when developing forest therapy programs or used the mechanisms or effects of previous studies, while 37 (64.9%) did not report information about the rationale for program development. Only 1 article (1.8%) reported that there is a manual to provide the same forest therapy program to the subjects. 29 articles (50.9%) reported the eligibility of the forest therapy program providers, 19 of which reported that the programs were run by forest therapy instructors. Others reported that forest therapy majors, forest commentators, art therapists, yoga instructors, specialized instructors, doctors, and nurses participated in running the programs. There were 28 articles (49.1%) not reporting information about program provider (Table 4).

Forest therapy program characteristics of included studies (N = 57)
Characteristics of forest therapy environments
There were 12 articles (21.1%) reporting both forest and thermal environments, which are therapeutic environments in which forest therapy programs were selected, while 15 (26.3%) reported only the forest environment. 30 articles (52.6%) did not report characteristics aside from the region or place name of the environment in which the program was provided. For forest environment, 21 articles reported about vegetation and tree types, 7 about the length of trails and altitudes, 5 about the structure of the forest such as slopes, 3 about phytoncide, and 1 each about negative ions, fine dust, and air pollution. For thermal environment, 12 articles reported about temperature, 7 about humidity, 6 about wind speed, 2 about illuminance, and 1 about average precipitation (Table 5).

Reported forest environmental factors of included studies (Include multiple reporting)
Discussion
This study was conducted to analyze the current state and characteristics of studies on the effects of forest therapy conducted in South Korea through a scoping review and to present concepts necessary for developing research methods to investigate the medical effects. A total of 564 articles were searched on 5 domestic and international databases, and 57 articles were ultimately analyzed.
Studies on the effects of forest therapy in South Korea have been conducted steadily since 2012, and show a sharp increase after 2020. This may have been because forest-based healing activities began to receive attention as an alternative to deal with the increased psychological health problems and decreased physical activity due to the COVID-19 pandemic, which increased social interest and led to an increase in forest therapy research (Ribeiro et al., 2021; Robinson et al., 2021; Soga et al., 2021). Regarding the concept of effect used in studies on the effects of forest therapy, 5 articles provided specific contents about symptoms or effects, and 52 articles used terms with comprehensive concepts of forest therapy programs such as 'verifying the effect of health promotion', 'physiological and psychological effect', 'effect on psychological health', 'effect on mental health', 'physical effect', and 'positive effect'. Hypotheses and purposes used in clinical research must be clear and provided in verifiable sentences to solve the problems (Chang et al., 2012). Although ambiguous or general expressions must be avoided when describing the research purpose, the studies on the effects of forest therapy analyzed here used many terms with broad meanings in the purpose, such as 'health promotion', 'psychological health', and 'positive effect', as well as vague expressions such as 'impact' and 'effect'. This may reduce the clarity of research and is not appropriate for research purposes to prove medical effects. One example of a specific expression used in clinical research can be: "This study will verify whether there is a significant decrease in depressive symptoms measured by the change in the total score of the OO depression scale by conducting A intervention N times." To verify the medical effects of forest therapy, it is necessary to use more specific and verifiable sentences to express which actions of forest therapy are effective, how effective they are, and for which symptoms they are effective, and then to investigate these effects through research.
Studies on the effects of forest therapy are clinical research involving humans, which is why ethical considerations are essential and of the greatest importance (Manton et al., 2014). In order to have medical evidence, it is necessary to clarify that studies on the effects of forest therapy are clinical research and to preemptively take ethical measures to respect and protect the subjects through deliberation of the IRB prior to research. The United States requires IRB deliberation of studies on human subjects funded by the Department of Health and Human Services. Moreover, the International Committee of Medical Journal Editors (ICMJE) specifies that articles published in medical journals must include provisions related to consent forms in their submission regulations and protect the research subjects (International Committee of Medical Journal Editors, 2023). This can be related to the fact that IRB deliberation was reported in all articles searched on international databases. South Korea has been making it mandatory to follow the related regulations in the Bioethics and Safety Act since 2013 (Kim and Kim, 2014), and the Korean Association of Medical Journal Editors (KAMJE) is also following the regulations of the ICMJE. Therefore, to obtain validity of medical evidence in the results of studies on the effects of forest therapy, it is necessary to have awareness about the importance of IRB deliberations and increase recommendations for IRB approval.
Scientific considerations are required from the research design in order to obtain valid conclusions in clinical research. To begin with, it is necessary to calculate the sample size using statistical power and the size of the confidence interval to select the sample size. In this study, we discovered 7 articles conducted by applying this process, and 87.8% of the studies did not involve the process of sample size selection. This may suggest that researchers are not aware of the importance of calculating sample size in studying the effects of forest therapy. If there is an insufficient sample size in clinical trials, desired results might not be obtained even if the study is rigorously conducted, or might lack reliability. On the other hand, a sample size that is too large can be inefficient in terms of time and cost and may incur difficulties in management, which is why the process of calculating sample size is an essential part of research design (Lee et al., 2013). To obtain valid results, it is necessary to promote awareness of the importance of calculating appropriate sample size for research and apply this to research design. Moreover, since effect size in clinical comparisons is the result of differences in the intervention applied to the experimental group and the control group, it is necessary to select research subjects rigorously, set the control group, and carefully select interventions provided to the control group in order to clearly identify the effects (Park, 2005).
There are various types and methods of clinical research as well as different levels of evidence depending on the research method. RCTs are considered to have the highest level of evidence and are perceived as the gold standard for evaluating effectiveness. On the other hand, before-after studies do not have a high level of evidence and thus also do not have much impact in proving effects (Evans, 2003). However, in the analysis of this study, there were 28 before-after studies comparing before and after the programs, accounting for 49.1% of all studies, while RCTs accounted for only 19.3%, which is less than half of the before-after studies. The reason why many before-after studies were conducted on the effects of forest therapy might be related to the development method of forest therapy programs. Forest therapy programs are commonly developed using instructional system development (ISD). This process consists of analysis, design, development, implementation, and evaluation, in which the developer sets the goal and organizes and delivers the program to achieve the goal (Kim, 2015). This program is evaluated by analyzing the level of goal attainment and changes in attitude through the before-after surveys and the satisfaction after the program with the purpose of systematically investigating the value and benefits of the educational process and outcomes (Ahn et al., 2003). It is reasonable to use program effectiveness evaluation through before-after comparison as the evidence for a wellness experience program. However, it is difficult to evaluate clinical safety and effectiveness for medical evidence of treatment support activities with such before-after studies. Clear evidence of therapeutic effects is needed in order for forest therapy programs to be used as treatment support activities, and forest therapy programs must be organized based on evidence. However, there is currently insufficient research on forest therapy that reveals specific and clear therapeutic effects and mechanisms of action through an adequate control group like RCTs, which is why there are limitations in organizing forest therapy programs based on evidence. Thus, it is necessary to first consider implementing RCT, a research method that can clearly compare effects, to create medical evidence for forest therapy. However, for studies conducted in the communities, it might be difficult to randomize all situations for ethical reasons (Bader et al., 2023). For this reason, efforts must be made to minimize the risk of bias that causes research errors when designing non-RCTs (Morgan et al., 2019; Furuya-Kanamori et al., 2021). These efforts are also known to improve the level of evidence (Kim et al, 2022).
Reproducibility of research is an important criterion that distinguishes science from non-science in research (Open Science, 2012, 2015), claiming that if the study results are real, the same results must be obtained by following the same procedures regardless of which researcher conducts the research (Simons, 2014). Among the articles analyzed in this study, there were none in which it is possible to reproduce the intervention effect with only the information provided. In order for the effects of forest therapy to have reproducibility, it is essential to report study results so that they are reproducible. As a result of this study, there were no studies reporting that the effects could be reproduced or that there was reproducible information for both the content of the program provided and the forest environment. If the information about the intervention provided in the study is unclear or limited, it is impossible to reproduce the study results or extend the study based on the results. Moreover, studies may be conducted redundantly when implementing interventions in different populations or settings, thereby wasting time and cost. Above all, it has been reported that limitations in intervention information may cause difficulties in the process of synthesizing study results such as systematic reviews analyzing medical effects (Campbell et al., 2018). In particular, programs used in forest therapy are complex interventions influenced by various components, environmental factors, program implementation, provider capabilities, and economic considerations (Skivington et al., 2021). Since complex interventions are affected by many variables, using just effect evaluation provided in the results is not enough for explaining the changes on the human body or the mechanisms of action (Craig et al., 2013). For this reason, international journals recommend the use of reporting guidelines for intervention studies such as TIDieR to enable reproduction of the interventions in studies providing interventions such as forest therapy programs (Hoffmann et al., 2014).
In forest therapy, selecting the forest environment is a key factor in maximizing the therapeutic effect along with organizing the program. A well-created forest environment is known to have a therapeutic effect just by being exposed to it (Park et al., 2010). However, the concentration and composition ratio of phytoncide, thermal environment, vegetation composition, and landscape constantly change in in forests depending on the season, which indicates that the healing elements that affect the human body also change (An et al., 2022; Kim et al., 2017; Park et al., 2017). In particular, Korea is a country with four distinct seasons with diverse landscapes and thermal comfort for each season, which result in diverse responses of the human body (Kim et al., 2019; An et al., 2022; Song et al., 2022). Accordingly, reporting the environmental conditions for the programs is as important as reporting the programs in detail to reproduce the effects of forest therapy. In order to predict and reproduce the effects of forest therapy, it seems necessary to discuss how to clearly report the contents of the therapeutic forest environments.
To evaluate medical effects, it is necessary to define which activities were provided, in what environment they were provided, to what extent they were provided, and for what. The effects of these activities must also be examined to organize the suitable forest therapy programs for each disease. Reporting on forest therapy programs and forest therapy environments to enable reproduction of effects along with rigorously designed clinical research is an essential element to clearly analyze the effects of forest therapy in research, and it is also absolutely necessary for the programs to be applied to health and medical care such as therapeutic support. Cumulative research that reports the contents of forest therapy programs and forest environments according to intervention reporting guidelines can be used as important evidence and data to develop programs suitable for therapeutic purposes in the future.
The contents that must apply the clinical research methodology presented for studies on the effects of forest therapy thus far can be summarized as shown in Table 6.

Considerations for applying clinical research methodology
'Medical evidence' presented by the Health Insurance Review and Assessment Service indicates the valid clinical research results that enable optimal use of health and medical care interventions (health technology), which mostly refer to evidence based on literature (Health Insurance Review and Assessment Service, 2020). Since the strength and validity of research evidence are evaluated based on the type of study, quality of literature (research bias), amount of evidence, consistency of evidence, and directness of evidence, it is necessary to improve quality of the literature with a rigorous experimental design to increase the level of medical evidence, and to report the study for reproducibility and confirm the reproduction of effects.
It is stated that health technology assessment institutions assess clinical safety and effectiveness using a systematic review to evaluate medical effects. A systematic review is a research method that collects and analyzes clinical literature results available at the point of evaluation based on an evaluation plan to answer specific research questions, and the analysis results vary depending on the validity and level of evidence in the clinical literature obtained (Ministry of Health and Welfare, 2022). In other words, to investigate the medical effects of forest therapy, there is a need for research design with a high level of evidence and rigorously conducted clinical research. This is because these study results can be synthesized and considered to have clinical safety and effectiveness.
This study analyzed and broadly explained the concept of effect, research methods, and characteristics of forest therapy programs and environments in domestic studies on the effects of forest therapy through a scoping review based on the clinical research method. Through this, we identified the trends in studies on the effects of forest therapy and proposed ways to apply the clinical research method of forest therapy to increase the levels of medical evidence. However, this study has limitations in that it reviewed literature with focus on scientific journals and thus may not have included literature such as theses, dissertations, or government reports.
Conclusion
This study conducted a scoping review by analyzing 57 articles that investigated the effects of forest therapy programs implemented in South Korea, which were published in domestic and international journals from 2012 to May 2023.
The following results were obtained by analyzing the selected literature. Studies on forest therapy have been conducted steadily since 2012 and have shown a sharp increase since 2020 after the outbreak of COVID-19, most of which were conducted on adults without diseases. 80.7% of the studies reported that ethical considerations were made through IRB deliberation and research consent, and 12.3% were conducted by calculating the sample size. Most studies were before-after studies, followed by non-RCTs and RCTs. There were insufficient reports about the contents of forest therapy programs for reproducibility of the effects of forest therapy. For forest therapy environments, 21.1% of the studies reported both forest and thermal environments, while 26.3% reported only the forest environment, indicating that more than half of the studies were not reporting about forest therapy environments.
The following suggestions can be made based on these results. First, to obtain validity in medical research on forest therapy, it must be clear that studies on forest therapy are clinical research, thereby ensuring respect and protection of the research subjects, and there is also a need for education and application of the clinical research method afterwards. This is necessary to extend rigorous research that can plan clinical trials with a high level of evidence from the research planning stage and minimize research bias. Using research report guidelines and risk of bias assessment tools that are widely used in international medical research might be helpful in this process. Furthermore, it is necessary to discuss essential items for report in the programs and forest environments and develop and apply reporting methods in order to increase the reproducibility of forest therapy programs that have the characteristics of a complex intervention.
Studies on the effects of forest therapy that have been conducted thus far through the efforts of many researchers have contributed greatly to revealing the concept of forest therapy and developing forest therapy so that it is established today as forest-based wellness. It is clear that existing studies on the effects of forest therapy have played a critical role in making forest therapy what it is today. However, in order for forest therapy to develop into a treatment support activity beyond just wellness, it is necessary to consider applying research methods to increase the level of research evidence while also making efforts to reveal medical effects. Applying medical clinical research methods to studies on the effects of forest therapy can improve the level of research evidence and develop the academic grounds for forest therapy, thereby laying the foundation for securing medical evidence that can develop forest therapy into a treatment support activity in health and medical care.